


Abstract
Objective To better understand the messages that family medicine residents receive about enhanced skills fellowship programs throughout their training.
Design Phenomenologic approach using structured qualitative interviews.
Setting Postgraduate family medicine program in Ontario.
Participants Eleven family medicine residents (5 first-year and 6 second-year residents) from 4 separate training sites.
Methods Interviews were audiotaped and codes were developed by the study investigators. Themes arose from the data via the immersion and crystallization technique.
Main findings Themes emerged in 3 categories: perception of purpose, sources of messaging, and formal or informal versus hidden curricular messages. Fellowship programs were viewed by residents in terms of their personal and professional benefits. Residents learned about fellowship programs through word of mouth and from role models. The formal curriculum remained neutral about fellowship training. The hidden curriculum highlighted a number of messages: a) to maximize chances of acceptance into some fellowship programs, one should focus most of his or her elective time in that clinical area; b) many fellowships graduate subspecialists to the exclusion of family medicine; c) a fellowship is required to practise in a large urban centre but is not required to practise in rural communities; and d) those without fellowship training are less well regarded.
Conclusion Residents receive mixed messages regarding fellowship training. This might be a phenomenon isolated to a larger urban centre in Ontario. Decision making at the individual level in terms of career path seems to be affected and might have implications at the larger system level.
As Canadian health care needs evolve, we have sought out ways to shape family medicine postgraduate education to best meet these needs. Strategies have included the development of northern and rural-specific programs,1 distributed medical education,2 and the development of enhanced skills training programs.3 These family medicine enhanced skills programs are offered to those residents who wish to obtain added competency in specific areas of focus.4 Enhanced skills programs now constitute an increasing component of Canadian postgraduate medical education in family medicine (21% of graduates pursued extended training in 2013 compared with 11% in 1995).4 This is consistent with the most recent 2014 National Physician Survey, wherein 32.4% of family physicians self-identified as those with a focused practice—a number that has also increased over time (29.5% in 2007, 30.5% in 2010).5–7 The messaging from the College of Family Physicians of Canada is clear that the goal of fellowship training is to incorporate these areas of enhanced skills as part of continuing comprehensive care.4,8
Despite this, the literature suggests that subspecialization within family medicine is a growing trend.4,9–12 An Ontario-based survey of both resident and teacher perspectives on fellowship programs concluded that this trend was largely owing to resident factors including “greater remuneration, employability, lifestyle flexibility, and geographic mobility.”13 It also suggested that demand will continue to grow and that extra training was increasingly required within our changing health care system.13 In one study examining perspectives of Canadian family medicine residents and educators, some respondents suggested that the true generalist was becoming an endangered species.9 While the factors that influence the decision to pursue fellowship training and specialization within family medicine are multifactorial,13,14 the literature supports the importance of a resident’s postgraduate educational and clinical experiences on future practice intentions.2,13,15–17
However, little is known about residents’ perceptions and understanding of the messages related to fellowship programs delivered in the postgraduate curricular context. Improved understanding of their views can help us shape curricular messaging that supports a comprehensive primary care system that meets community needs. For this reason, the study objectives were to understand what residents believe to be the purpose of fellowship programs, identify their sources of information about enhanced skills programs, and describe the messages they receive from their program-related training.
METHODS
Study design
A qualitative phenomenologic approach was used to best understand the richness of the resident experience. Hospital-based ethics approval was granted by the University Health Network research ethics board before study commencement. A structured interview guide was developed by the research team (L.P., A.M., and C.H.) based on the study objectives in order to target identified gaps in the literature. (To retrieve a copy of the interview guide, contact the corresponding author [L.P.].) Qualitative interviews using this interview guide were then conducted by the study primary investigator (L.P.) with family medicine residents within an Ontario postgraduate family medicine program.
Recruitment and sampling
Residents were recruited using both criterion sampling (a program-wide e-mail was sent to all first- and second-year residents in family medicine in the postgraduate program) and, subsequently, snowball sampling until data saturation was reached. As this was an exploratory study, we chose purposive sampling based on this criterion only to target a range of experiences. Four separate training sites were represented (3 downtown sites and 1 community site, including rural stream participants).
Analysis
Interviews were audiotaped, transcribed, and anonymized by the primary investigator. Codes were developed independently by each member of the research team (a second-year resident at the time of writing [L.P.] and 2 staff physicians with diverse backgrounds [A.M., C.H.]) after thorough review of the transcripts and after consultation with a qualitative research scientist. When consensus was reached, transcripts were coded accordingly by the primary investigator and again reviewed and confirmed by the research team. The primary investigator, having conducted, transcribed, and coded all interviews, was completely immersed in the data, and key themes crystallized through this reflective process. Reflexivity was maintained through an iterative and conscious search for contradictory observations, as well as regular check-ins with all team members. Trustworthiness of data was ensured through data saturation, as well as triangulation of content and themes.
FINDINGS
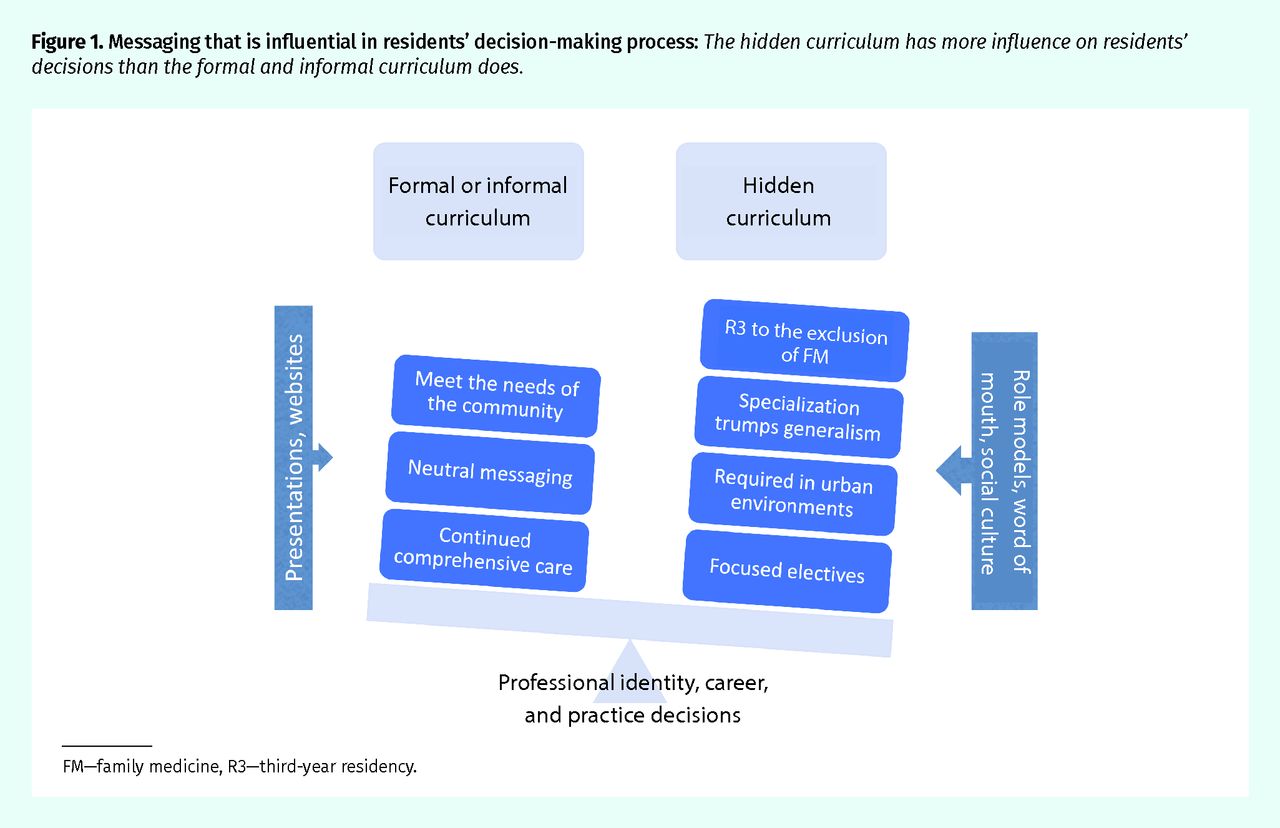
Eleven participants were interviewed: 6 first-year and 5 second-year residents; 4 were male and 7 were female. Three common themes emerged from the data: perception of purpose, sources of messaging, and formal or informal messages versus hidden curricular messages (Figure 1).

Messaging that is influential in residents’ decision-making process: The hidden curriculum has more influence on residents’ decisions than the formal and informal curriculum does.
FM—family medicine, R3—third-year residency.
Perception of purpose
Personal benefits over benefits to the community and the health care system.
Most residents emphasized that fellowship programs would allow them to pursue a personal interest by expanding their skill set, be more comfortable with independent practice in certain clinical environments, and prevent burnout.
Maybe one consideration is that it seems like more training would be helpful in terms of my own confidence, or skill set, whether actual or perceived. (R8)
I could see that potentially down the road if in 10 years from now I become a little burnt out with general practice, I may want to focus on something to make it easier for myself on a day-to-day basis. (R10)
To a lesser extent, some residents mentioned cost savings for the system, increased access for patients, and decreased wait times.
I think that it could be an ultimately lower-cost option …. The idea being that it is a family physician billing for certain services that are lower than what their specialty colleague would bill for similar consultation services. As well, if somebody is practising in a rural area, then if they avoid people having to be referred and transferred or sent to a bigger centre. (R8)
One resident pointed out a disconnect between the timing of the fellowship programs immediately following completion of family medicine training and their identified role in meeting community needs:
I remember in [province] they encourage people to go out and practise for a couple of years before doing that additional year of fellowship training. The idea being that then you have a sense of what your community needs you to have more skills in, and I really liked that. (R7)
Residents also touched on the systems issues related to fellowships becoming “shortcuts” to specialization.
You are saying we are training this number of residents to be able to meet the needs of the community and then the needs of the community aren’t met because 10% to 20% of those residents aren’t doing general family practice, they are doing more of a specialty focus; that is a problem. (R11)
Sources of messaging
Role models, word of mouth, and the influence of the informal curriculum.
Residents both planning and not planning on fellowship training believed that their decision was reinforced by working with and speaking to faculty and resident role models primarily via the informal curriculum (the opportunistic, unplanned instruction between a teacher and trainee).
Informally, when I see a lot of our physician mentors, many of them do have plus ones and do have a lot of experience in one specific area. If I were interested in more of the academic role, it makes me think that I would need to have more of a specialty or niche in family medicine. So I think it is kind of that informal, learning by osmosis ... by observing who the people are that are our teachers. (R9)
Word-of-mouth advice from mentors was viewed as influential.
They have done locums in more rural settings, have worked overseas, and their advice for me was ... they see a lot of residents using it [the fellowship] as a crutch. They say go out and practise, you’ll be OK, you’ll know enough. I took that pretty seriously. (R7)
Conversely, the lack of comprehensive family medicine role models in some environments was cited as contributing to a perceived pressure to pursue fellowship training.
The physicians who have these niche practices as well are the ones who are the leaders in the academic communities and are also the ones who are kind of revered for their research or other academic work. So, we maybe just don’t have as much exposure or as much highlighting of people who do true general comprehensive family medicine. (R8)
Curricular messages
Formal curriculum.
Formal curriculum examples were described to residents as including various educational formats such as formal didactic presentations; online resources; organized small group learning; and department-led, town hall–style events.
Undergraduate messages and planting the seed early: Formal undergraduate presentations related to fellowship training were cited as key to some residents deciding to pursue family medicine. The message from these presentations, as well as informal discussions with educators, was that increased flexibility could satisfy multiple clinical interests.
I guess having the opportunity for a fellowship in my back pocket as a way of kind of merging the 2 programs, like merging my interests in the subspecialty I wanted to do versus family .... It is a way to kind of ... it drew me in. (R3)
Back in med school when we were having family medicine interest groups and hearing about family medicine as a specialty, that was often the selling point. The idea that you can do these plus 1 year of additional training in obstetrics, or in palliative care, or in anesthesia. (R7)
Postgraduate messages as neutral: Residents unanimously believed that their postgraduate program’s formal curriculum was neutral regarding the issue of fellowship programs, and that it encouraged residents to be confident that they would be competent to begin comprehensive family medicine practice after 2 years of training.
I think it is framed more as there are lots of options that exist for fellowships. If you want to do them, that’s great. If you don’t want to do them, that’s also great, because we are giving you comprehensive training. (R7)
Despite existing resources, most residents believed there was a gap in the formal curriculum surrounding how to best prepare for a fellowship: “I feel like there is not a lot of information in terms of how many electives you actually have to do? What’s the process actually like? What’s the best way to network to get into this?” (R2)
Hidden curriculum.
The hidden messages that emerged within the postgraduate curriculum were not explicitly presented as part of formal or informal teaching but they exist within the educational social culture.
Improving success for acceptance: Many residents discussed a perceived need to complete numerous electives in the fellowship discipline to have a successful application. A few residents labeled this process as redundant and believed it might detract from comprehensive family medicine training. One resident explained the following: “Maybe they [residents] must really focus their whole 2 years of training on trying to get into the program rather than learning what they need to learn to be a family doctor.” (R8)
Integration of enhanced skills within comprehensive family medicine: Many residents believed that some fellowships served to train subspecialist physicians often to the exclusion of comprehensive family medicine. Palliative care and emergency medicine were often discussed as 2 exemplars.
I think it really serves to really focus kind of a niche practice .… Even palliative care, I feel like the fellowship … the impression that I’m getting is that you are becoming more of a palliative care physician, rather than doing family practice with some supplementary palliative care. (R2)
Although I think in a lot of ways, at least typically, the emerg program is just sort of seen as a way for people to become emerg docs in 3 years as opposed to 5 years. (R10)
“Just family medicine”: One of the loudest messages heard by the resident participants through the hidden curriculum was the idea that practising family medicine without enhanced skills training was viewed as lesser or lacking in some way. Residents believed this reflected a culture of specialization, and some found themselves defending their decision to practise family medicine without fellowship training.
It is this general thing that it’s not just that you’re doing family medicine for the 2 years, but you know, “Are you doing a PGY3?” is this automatic follow-up question. (R2)
I’ve found at the beginning there was this expectation that specialties are better, or more prestigious, or more high achieving than people who want to be generalists …. I think there should be a little bit more positive encouragement to be a generalist, which is what we are supposed to be. Sorry, not supposed to be ... but what we are … in theory, what we joined this program to be. (R6)
Rural and urban divide
Residents believed that there was a difference between larger city centres and rural communities in terms of the role of fellowship training. In the urban setting, residents viewed fellowships as a prerequisite to practising, or at least a considerable employment advantage:
If you want to practise in [city], maybe at even one of the teaching sites, if you wanted to practise some academic family medicine, then you would need some additional training. That is maybe less so people saying that you actually need the additional skills that you get, but more you need the certification. (R8)
In contrast, several residents thought that if one were to practise rurally, the message was essentially the opposite:
I would say maybe I’ve felt a little bit of ... I wouldn’t call it pressure I would just say a little bit of influence from people telling me that I don’t need to pursue a fellowship if I’m going to go work somewhere rural and that I could just gain these skills by hopefully learning from people in the community and practising. (R10)
DISCUSSION
Currently, the College of Family Physicians of Canada formally recognizes 19 programs reflecting an area of special interest or focused practice across the country while “remaining committed to comprehensive continuing care.”8 The formal messaging surrounding the purpose of enhanced skills fellowships at the national and local levels seems to be quite clear: they serve to fill gaps that exist within a community of practice and aim to function in concert with comprehensive family medicine rather than to its exclusion.4,8,18
Despite this, residents in this study, as well as in the literature, view fellowships primarily in terms of their potential personal and professional benefits.13 As residents are asked to make their fellowship application decisions well before most know their future practice environment, it might be difficult for them to truly understand where their community needs lie. To have a competitive application, residents understood that they must focus their clinical electives. This raised concern among residents about the possible loss of comprehensiveness in their training. Consistently, residents believed that several fellowship programs generate graduates who do not practise comprehensive family medicine. This perception is supported by Ontario physician billing data that confirm that graduates from emergency medicine fellowships practise exclusively or almost exclusively emergency medicine.10,19
The hidden curriculum was identified by residents in this study as more influential to their decision-making process than explicit messages heard through the formal and informal curriculum (Figure 1). This is supported by several additional studies that suggest the hidden curriculum is as important as, if not more so, (and is frequently at odds with) the formal one in terms of future effect and the development of a professional identity.9,20,21 In this study, the hidden curriculum created a cultural understanding among residents that 2 years of clinical training is often viewed less favourably or creates physicians who are less competent than those who pursue fellowship training. They also understood that pursuing a fellowship was advantageous, if not necessary, for urban academic centre practice. Residents believed that fellowships were less necessary in rural environments where they learn primarily through mentorship. This appears at odds with the health systems perspective, as these are environments where access can be limited to consultants and there is potential benefit to extra training.
There is a growing trend toward specialization within family medicine. A 2017 Ontario study based on administrative data showed that in 2014 to 2015 approximately two-thirds of primary care physicians practised comprehensive care, compared with 75% in 2003 to 2004. It also highlighted a disproportionate population growth and subsequent decline in availability of comprehensive family physicians.22 This decreases access to primary care, particularly for rural and remote communities, and poses potentially substantial health care resource management challenges in Canada.9,23 While the reasons for pursuing fellowship training are numerous, the unspoken messages described by residents in this study suggest a number of beliefs at odds with what is formally projected at both the local and national levels, which might serve to further promote specialization.
Limitations
Purposive sampling resulted in a broad group of residents that was diverse but not necessarily representative of the entire program. Despite efforts to maintain reflexivity, the identity of the primary investigator as a peer resident might have affected responses. Targeted sampling methods might help uncover experiences unique to urban versus rural residents, or at specific times in their training. More studies are needed across the country to determine whether the phenomena described in this paper might be applicable to other family medicine programs.
Conclusion
These results raise new questions about how family medicine enhanced skills fellowships are discussed, structured, and taught. Family medicine departments must critically look at the hidden curriculum (ie, the social structures, word-of-mouth messages, role models, and practice styles to which our residents are exposed during their training) and be proactive in addressing some of the messages that seem to exist within it. Nationally, we need to ensure that the opportunity and diversity offered through these special interests are not at the loss of comprehensive family medicine.
Acknowledgments
The study was undertaken as part of a family medicine residency research project at the University of Toronto.
Notes
Editor’s key points
▸ By understanding residents’ perceptions of the messages related to fellowship programs delivered in the postgraduate curricular context, we can shape curricular messaging to support a comprehensive primary care system that meets community needs.
▸ The formal messaging surrounding the purpose of enhanced skills fellowships is clear: they fill gaps that exist within a community of practice and aim to function in concert with comprehensive family medicine rather than to its exclusion. However, residents in this study viewed fellowships primarily in terms of their own personal and professional benefits.
▸ The hidden curriculum was identified by residents in this study as having a greater influence on their decisions than the explicit messages heard through the formal and informal curriculum. The hidden curriculum created a cultural understanding among residents that 2 years of clinical training is often viewed less favourably, or creates physicians who are less competent than those who pursue fellowship training. Residents also believed that pursuing a fellowship was advantageous, if not necessary, for urban academic centre practice. Residents thought that fellowships were less necessary in rural environments where they learn primarily through mentorship.
Points de repère du rédacteur
▸ En comprenant comment les résidents perçoivent les messages concernant les programmes de formation en compétences avancées qui circulent dans le contexte du cursus postdoctoral, nous pouvons formuler les messages du cursus de manière à promouvoir un système de soins primaires complets et globaux qui répond aux besoins de la communauté.
▸ Le message officiel entourant le but des programmes de formation en compétences avancées est clair : combler les lacunes qui existent dans une communauté de pratique donnée, et exercer en même temps une médecine familiale complète et globale plutôt que l’exclure. Toutefois, les résidents dans cette étude envisageaient ces programmes de formation en fonction de leurs avantages personnels et professionnels.
▸ Les résidents dans cette étude ont fait valoir que le cursus caché influait davantage sur leurs décisions que les messages explicites entendus dans le cursus formel et informel. Le cursus caché a créé une impression culturelle chez les résidents selon laquelle une formation clinique de 2 ans est souvent vue moins favorablement, ou produit des médecins moins compétents que ceux qui suivent une formation en compétences avancées. Les résidents croyaient aussi que la formation en compétences avancées était avantageuse, voire nécessaire, pour la pratique dans un centre universitaire urbain. Les résidents pensaient que la formation en compétences avancées était moins nécessaire dans les milieux ruraux, où ils apprennent principalement par le mentorat.
Footnotes
Contributors
Dr Payne was the principal investigator of the study and the primary lead on all aspects of the project; she decided on the methods, developed the study tools, recruited and interviewed participants, transcribed the interviews, analyzed the data, developed the final themes, and wrote and edited the manuscript. Dr Moaveni was involved in the development of the study purpose and methods, and analysis of the data; worked closely with Dr Payne in developing the codes and final themes; and contributed to editing multiple draft copies of the manuscript. Dr Handford was heavily involved at the onset of this study, helping to select the best methodology with which to answer the research question; he edited the interview guide, assisted in the analysis of data (development of codes and final themes), and contributed to editing multiple draft copies of the manuscript before finalization. Drs Moaveni and Handford supervised Dr Payne directly throughout the duration of the project.
Competing interests
None declared
This article has been peer reviewed.
Cet article a fait l’objet d’une révision par des pairs.
- Copyright© the College of Family Physicians of Canada
References
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- Une integration novatrice pour aller de lavant: Un programme de 3 ans de residence en medecine familiale et en competences avancees
- A new way forward via innovative integration: A 3-year family medicine and enhanced skills residency program
- Valuing our past, sustaining our future: Generalists of tomorrow