


Abstract
Objective To identify the mechanisms associated with success and failure of chronic disease prevention and management (CDPM) programs, as well as their key contexts.
Design Realist synthesis.
Setting Six primary care CDPM programs funded between 2011 and 2013 in Quebec.
Participants Patients, health providers, program leaders, and other stakeholders involved in CDPM programs.
Methods A collaborative research process was implemented, involving representatives from the executive and advisory committees: researchers, health care providers, decision makers, and patients and families. Leaders were asked to provide all documents related to their programs to the research team. The documents were selected depending on their relevance and rigour. The thematic analysis of each program consisted of identifying the outcomes and mechanisms, as well as the specific contexts associated with these outcomes. Results for each program were validated by its leader before synthesizing the results of all programs together.
Main findings A total of 108 documents (eg, grant applications, scientific reports) were collected from the programs. Positive and negative outcomes were observed at the patient, health care provider, and health care system levels. Four main mechanism categories were associated with outcomes: patient-centred interdisciplinary care; self-management support and a motivational approach; professional support; and care coordination and relationships with partners. The main contextual factors that influenced the successes of these mechanisms were related to patients (multimorbidity, involvement of family caregivers), to health care providers (professional training, culture of interprofessional collaboration, mobilization of family physician), and to health care organizations (coordination between services, history of collaboration between partners, funding).
Conclusion This study confirms the essential role of patient-centred interdisciplinary care; self-management support and a motivational approach; professional support; and care coordination and relationships with partners when caring for patients with chronic diseases. It constitutes a relevant contribution for stakeholders involved in primary care transformation and should be used to inform the sustainability and scaling up of CDPM programs.
Chronic diseases represent a considerable challenge for the health care system1 owing to their prevalence, their direct and indirect costs, and their effects on patient health outcomes and quality of life.2 Many people living with chronic disease have multiple chronic conditions (multimorbidity),1,3 complex self-care needs, and challenging continuity of care.4,5 In Quebec, one-quarter of the population aged 12 and older had at least 2 chronic health problems in 2010 to 2011.6
The Quebec Ministry of Health and Social Services has made chronic disease prevention and management (CDPM) a priority by developing a reference framework for CDPM based on the chronic care model (CCM).7,8 The purpose of this framework was very broad: to advocate CDPM as a key feature of primary care, to support best practices in relation to CDPM, to better integrate CDPM into a continuum of services, and to mobilize all stakeholders concerned with chronic diseases.9
In 2011, Fonds de recherche du Québec – Santé, the provincial health research funder,9 in partnership with the Quebec Ministry of Health and Social Services and Pfizer launched a funding initiative to support innovative projects for CDPM, driven by local health organizations in collaboration with health researchers.9,10 Seven CDPM programs in Quebec received funding from 2011 to 2013 to allow the implementation and evaluation of these projects.11,12 The purpose of this study was to identify the mechanisms associated with success and failure of these CDPM programs, as well as their key contexts.
METHODS
The realist synthesis approach was chosen to embrace the heterogeneity and complexity of the programs’ publications and gray literature,13 and to synthesize evidence from the Quebec context, programs, and knowledge transfer meetings. Realist synthesis is a novel and innovative theoretically driven qualitative approach for reviewing and synthesizing quantitative and qualitative evidence from complex interventions.14 The realist synthesis approach is well suited to addressing the main research question and overarching objective of our research synthesis because it provides valuable insight into how and why programs lead to change, as well as for whom and in what context.15 It can generate transformable lessons to help practitioners and decision makers roll out or scale up a program intervention.16,17
This synthesis used the 5-stage iterative approach described by Pawson: 1) clarifying the scope of the realist synthesis; 2) searching for the evidence and appraising the evidence; 3) extracting and analyzing the data; 4) synthesizing the findings; and 5) disseminating the results.15 Adaptations to the traditional realist synthesis approach were made in regard to our decision to examine only CDPM programs in 1 particular context, as different health systems might be influenced by different contextual factors such as health care funding or primary health care reform, and our search strategy to identify the evaluation materials of the examined CDPM programs.
An executive committee and an advisory committee were created to ensure governance of the research and representativeness of all stakeholders (Table 1). The research team agreed on key terms, based on literature on realist approaches (Table 2).18–20 These terms were clarified for committee members in order to develop a common understanding. As the CCM was the theory underpinning all programs, the committees agreed on using the components of the CCM as the first version of the analytic grid.
Mandate and composition of the executive committee and the advisory committee
Definitions of context, mechanism, outcome, and CMO configuration
Program leaders were asked to provide all documents related to their programs: peer-reviewed publications, gray literature, including scientific reports, grant applications, program presentations, press releases, and documentation on the results and effects of the program. These documents were critically assessed by 2 team members against 2 criteria: relevance (appropriateness and richness of the content in terms of outcomes, contextual elements, mechanisms, program theory, and general understanding of the program) and rigour (whether the documents and the program evaluation were appropriate to generate credible and trustworthy data). Only those documents meeting these criteria were selected for analysis. At this stage, members of 1 program declined further participation; therefore, the realist synthesis was based on the remaining 6 programs.
An iterative and interpretative thematic analysis of documents was conducted independently by 2 research assistants in order to extract relevant data and synthesize the data into context-mechanisms-outcome (CMO) configurations: identification of outcomes; identification of mechanisms and contexts associated with the outcomes (if needed, new mechanisms were added to the initial analytic grid); classification of outcomes among 3 levels (ie, patient, provider, and organization); and synthesis of the data in the form of all CMO configurations found in each program. Discrepancies or disagreements between the research assistants were systematically discussed with the co-authors to reach a consensus. Chronic disease prevention and management program leaders were contacted to validate the results related to their programs.
Finally, the CMO configurations from each of the 6 programs were synthesized into 1 unique table and presented to the executive and advisory committees. Mechanisms from the initial analytic grid that had no link to outcomes were not retained. Main mechanisms and contexts involved in the CMO configurations were selected. They were chosen by applying the following principles: Mechanisms had to be found in 2 or more programs, with outcomes present at 2 or more levels (ie, patients, providers, or organization). The identified context had to be linked to 3 or more mechanisms; alternatively, contexts must have been associated with unexpected and important outcomes.
An integrated knowledge translation plan was put in place and included the following: a knowledge exchange meeting with all programs, a formal written report, several presentations during conferences,21,22 and this publication.
FINDINGS
A total of 108 documents were collected (Table 3). Nearly half of the documents pertained to the results of programs. The rest included descriptions of the programs and their implementation.
Documents collected
Outcomes
Outcomes at the patient level were mainly related to access to CDPM services, complementary resources, or secondary care, as well as health status, quality of life, disease self-management, and satisfaction. Outcomes at the provider level pertained to the degree of interprofessional collaboration, workload, and knowledge and satisfaction. Finally, outcomes at the organizational level related to access to health services, coordination of care, involvement of family physicians, and partnerships among stakeholders of the local health services network.
Contexts, mechanisms, and outcomes
Twenty-one mechanisms were involved in the identified CMO configurations; among them, 11 main mechanisms were selected and linked to 4 out of the 6 components of the CCM (Table 4). Nineteen contexts were identified and 10 of them were selected as main contexts (Figure 1). Here we present the identified CMO configurations by the mechanism category.
Mechanisms identified and their relation to the CCM: The 11 main mechanisms are in boldface.
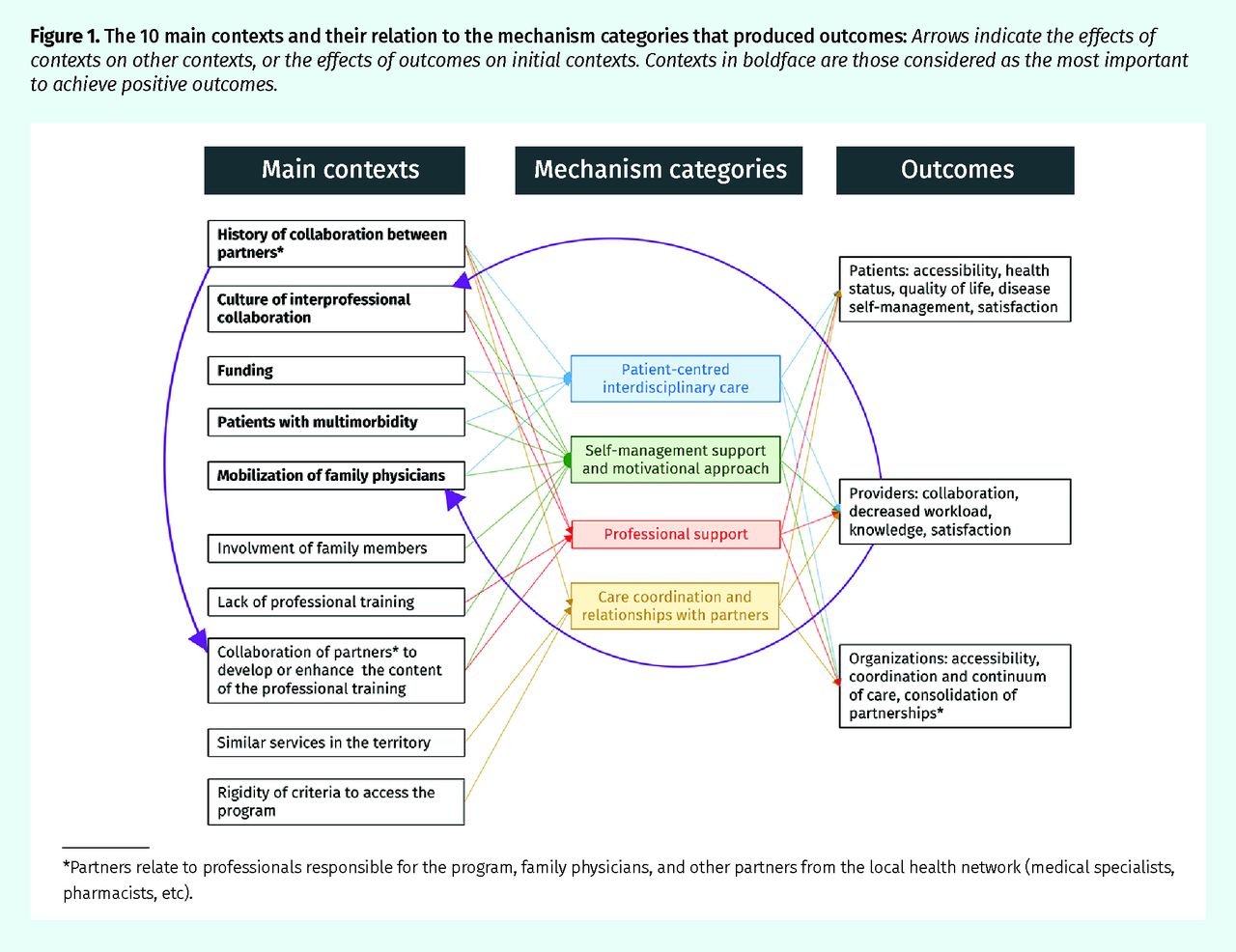
The 10 main contexts and their relation to the mechanism categories that produced outcomes: Arrows indicate the effects of contexts on other contexts, or the effects of outcomes on initial contexts. Contexts in boldface are those considered as the most important to achieve positive outcomes.
*Partners relate to professionals responsible for the program, family physicians, and other partners from the local health network (medical specialists, pharmacists, etc).
Patient-centred interdisciplinary care.
Patient-centred interdisciplinary care was mainly associated with positive outcomes for patients, providers, and organizations. Outcomes for patients included improved access to services, health status, quality of life, disease self-management, and satisfaction. Outcomes for providers included improved interprofessional collaboration, decreased workload, and increased satisfaction. Outcomes for organizations included improved care coordination. In 2 programs negative outcomes were also observed: limited access to services, limited involvement of family physicians, and increased workload among professionals. Regarding contextual factors, an established collaboration among family physicians, program leaders, and partners of the local health services network had a positive effect on patient referral and on mobilization of family physicians. Financial incentives also positively affected recruitment and effectiveness of the programs, as well as some characteristics of the patients, such as multimorbidity.
Self-management support and a motivational approach.
The outcomes associated with self-management support and a motivational approach at the 3 levels were as follows: increased access to services and improvement in motivation, health status, health behaviour modifications, quality of life, and self-management skills, as well as increased satisfaction, at the patient level; improvement in interprofessional collaboration, decreased workload, and increased satisfaction at the provider level; and improved access to CDPM services and quality of care at the organizational level. This was facilitated by the same favourable context as for patient-centred interdisciplinary care, as well as by the involvement of patients’ family caregivers and by the constitution of a co-located interdisciplinary team. In 1 program, some members of the interdisciplinary team collaborated to enhance the content of the professional training, and this was related to providers’ better appropriation of the intervention and finally to patients’ positive outcomes.
Professional support.
Professional support was associated with several positive outcomes at all 3 levels: improved self-management, health behaviour modifications, and health status at the patient level; acquisition of knowledge, improved self-efficacy, and decreased workload at the provider level; and strengthened links between partners of the local health services network, harmonized practices, and improved quality of care at the organizational level. This was facilitated by a culture and history of collaboration among partners of local health services networks. Positive outcomes were also observed when members of the interdisciplinary teams collaborated to develop the clinical content of the training. The positive outcomes observed helped change initially unfavourable program contexts, such as lack of professional training.
Care coordination and relationships with partners.
The positive effects associated with this mechanism category among the 3 levels included the following: improved access to primary and secondary care services at the patient level; increased satisfaction and enhanced collaboration at the provider level; and improved coordination of care and strengthened links among partners of the local health services networks at the organizational level. A history of collaboration between actors in the local health services network, family physicians, and medical specialists was the main positive context identified. In 2 programs, negative outcomes were observed: limited recruitment of patients for the program, limited access to complementary resources, and low consolidation of links among the partners of the local health services network. The contexts associated with these outcomes were as follows: existence of current services similar to those offered by the program, “rigidity” of the criteria to access to program services, and difficulties in mobilization of partners of the local health services network owing to lack of collaboration and of funding.
Other mechanisms.
Three programs planned the systematic integration of information into the patient medical record. Two programs planned the constitution of a chronic disease regional registry. Contextual factors, including financial aspects, seemed to have limited the implementation of these mechanisms related to clinical information systems. This resulted in negative outcomes, such as increased workload and professional dissatisfaction, at least during the implementation of these information systems.
Finally, several programs had mechanisms related to using community resources. Only 1 program implemented the mechanism (partnership with a private physical activity centre) and generated positive outcomes for patients and for organizations, in a context characterized by specific funding, a history of collaboration, and integration of community partners into the program.
DISCUSSION
This realist synthesis helps understand how CDPM programs work in different contexts. For future programs, it provides cues on the main mechanisms to recommend, as well as on the main contexts to take into consideration. Decision making should be informed by evidence that really reflects “real world practices.”23 Our synthesis is grounded in the knowledge, expertise, and first-hand experience of real-world patients, providers, program leaders, and other stakeholders involved in CDPM programs.
Our results are broadly in line with the holistic principles found in various chronic disease management models: the CCM,24,25 the extended CCM,26 the patient-centred medical home,27 the patient-centred approach,28,29 the multimorbidity approach,30 and self-management support.31,32 Patient-centred care and self-management support for people living with chronic diseases have been associated with improvement in terms of patients’ behaviour, satisfaction, health status, and health care use, as well as quality of care and providers’ satisfaction.33–35 The constitution of a co-located interdisciplinary team, close to a patient’s living environment, has been much less evaluated to date.36,37 This mechanism has the potential to increase patients’ access to CDPM services, to involve and support patients and their families in more depth and for a longer term, to contribute to the development of a shared vision between the care providers, and to better integrate care for patients.38 The importance of care coordination has already been highlighted in chronic care.39 Higher coordination of care can improve patient access to services, decrease obstacles to professional collaboration, and facilitate transitions of care for patients.40 Previously published literature has also highlighted the importance of professional support and training, especially in terms of interprofessional care and self-management support, to improve care for those living with chronic diseases.41,42
Knowledge about contextual factors that can influence the implementation and effects of these promising mechanisms is essential for any stakeholder involved in CDPM programs. Most publications related to intervention studies based on the CCM lack details about the interventions and their context.43 Literature on contextual factors is scarce,23,43,44 and our results constitute an original contribution in this regard.
Limitations
This synthesis has limitations. First, it focused on programs implemented in Quebec only. However, many provinces and countries face similar challenges in terms of chronic disease prevalence and health care system transformations. The approach used in this synthesis makes it easy for readers to assess for similarities or differences with their own context, thus ensuring some relevance for stakeholders from many countries. Second, the results depend on the number and richness of the documents analyzed. Despite our efforts to complete the data collection, including repeated calls to program leaders for new documents during the research process, data might have been incomplete for some programs. Finally, our work is based on an interpretative process. On the other hand, it brings the perspectives of many disciplines involved in primary care.
Conclusion
Understanding how CDPM programs work in different contexts is essential knowledge for health professionals, decision makers, and other stakeholders who want to improve care for patients with chronic disease. In light of this synthesis, patient-centred interdisciplinary care; self-management support and a motivational approach; professional support; and care coordination and relationships with partners are associated with positive outcomes for patients, providers, and organizations, depending on the context where such programs are implemented. A history and culture of collaboration, funding, characteristics of the patients, mobilization of family physicians, and involvement of family members seem to be particularly important factors to consider. These results constitute an original and relevant contribution for all stakeholders involved in primary care transformation and could be used to inform the sustainability and scaling up of CDPM programs.
Acknowledgments
The study was funded by Fonds Pfizer, Fonds de la Recherche du Québec – Santé, and the Ministère de la Santé et des Services sociaux maladies chroniques. Fonds de la Recherche du Québec – Santé peer reviewed the protocol and managed the funds. None of the funding entities had any role in preparing, reviewing, or approving the manuscript. We acknowledge the contribution of all program leads, as well as all health care professionals, decision makers, patients, and family members.
Notes
Editor’s key points
▸ Understanding how chronic disease prevention and management (CDPM) programs work in different contexts is essential for improving care of patients with chronic disease. As CDPM has been made a priority in Quebec, several CDPM programs in the province received funding for the implementation and evaluation of CDPM-supporting projects. The purpose of this study was to identify the contexts, mechanisms, and outcomes associated with these CDPM programs.
▸ Patient-centred interdisciplinary care; self-management support and a motivational approach; professional support; and care coordination and relationships with partners were associated with positive outcomes for patients, providers, and organizations, depending on the context where programs were implemented. A history and culture of collaboration, funding, characteristics of the patients, mobilization of family physicians, and involvement of family members seemed to be particularly important factors to consider.
▸ Outcomes at the various levels included improvement in health status, quality of life, and disease self-management (patient level); improved interprofessional collaboration and decreased workload (provider level); and improved access to health services, coordination of care, and involvement of family physicians (organization level).
Points de repère du rédacteur
▸ Il est essentiel de comprendre le fonctionnement des programmes de prévention et de prise en charge des maladies chroniques (PPCMC) dans divers contextes pour améliorer les soins aux patients qui en souffrent. Parce que les programmes de PPCMC sont considérés comme prioritaires au Québec, certains d’entre eux y ont reçu du financement pour mettre en œuvre et évaluer des projets à l’appui de la PPCMC. Cette étude avait pour but de cerner les contextes, les mécanismes et les résultats associés à ces programmes de PPCMC.
▸ Des soins interdisciplinaires centrés sur le patient; le soutien à la prise en charge autonome et une approche motivationnelle; le soutien professionnel; et la coordination des soins et les relations avec les partenaires étaient associés à des résultats positifs pour les patients, les professionnels et les organisations, selon le contexte dans lequel ces programmes étaient mis en œuvre. Des antécédents et une culture de collaboration, le financement, les caractéristiques des patients, la mobilisation des médecins de famille et l’implication des membres de la famille semblaient être des facteurs particulièrement importants à prendre en compte.
▸ Sur les divers plans, les paramètres étudiés étaient l’état de santé, la qualité de vie et la prise en charge autonome (niveau du patient); l’amélioration de la collaboration interprofessionnelle et la diminution de la charge de travail (niveau du professionnel); et un meilleur accès aux services de santé, la coordination des soins et l’implication des médecins de famille (niveau organisationnel).
Footnotes
Contributors
Dr Ramond-Roquin took the leadership for the writing of the paper as a postdoctoral fellow under the supervision of Dr Fortin. Drs Fortin and Chouinard designed the study. All authors conducted the analysis, contributed to the first manuscript draft, had full access to the data, and take responsibility for the integrity of the data and the accuracy of the qualitative analysis. All authors contributed to the writing and gave final approval of the present version. Dr Fortin takes responsibility for the integrity of the work as a whole.
Competing interests
None declared
This article has been peer reviewed.
Cet article a fait l’objet d’une révision par des pairs.
- Copyright© the College of Family Physicians of Canada
References
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.