


A similar number of men and women have epilepsy.1,2 However, the use of antiseizure drugs can be more complicated in women for various reasons. For example, hormonal changes can affect seizure control and the metabolism of antiseizure drugs, and there are many interactions between antiseizure drugs and hormonal contraception. Antiseizure drugs can also increase the risk of osteoporotic fractures later in life3 and increase the risk of birth defects if taken during pregnancy.2,4 To support clinicians in caring for women who take antiseizure drugs, we developed a patient-friendly infographic. The infographic focuses on 2 topics: the use of antiseizure drugs in pregnancy and breastfeeding (Figure 1)* and antiseizure drug interactions with hormonal contraception (Figure 2). Both figures are also available from CFPlus.*

Antiseizure drugs in pregnancy
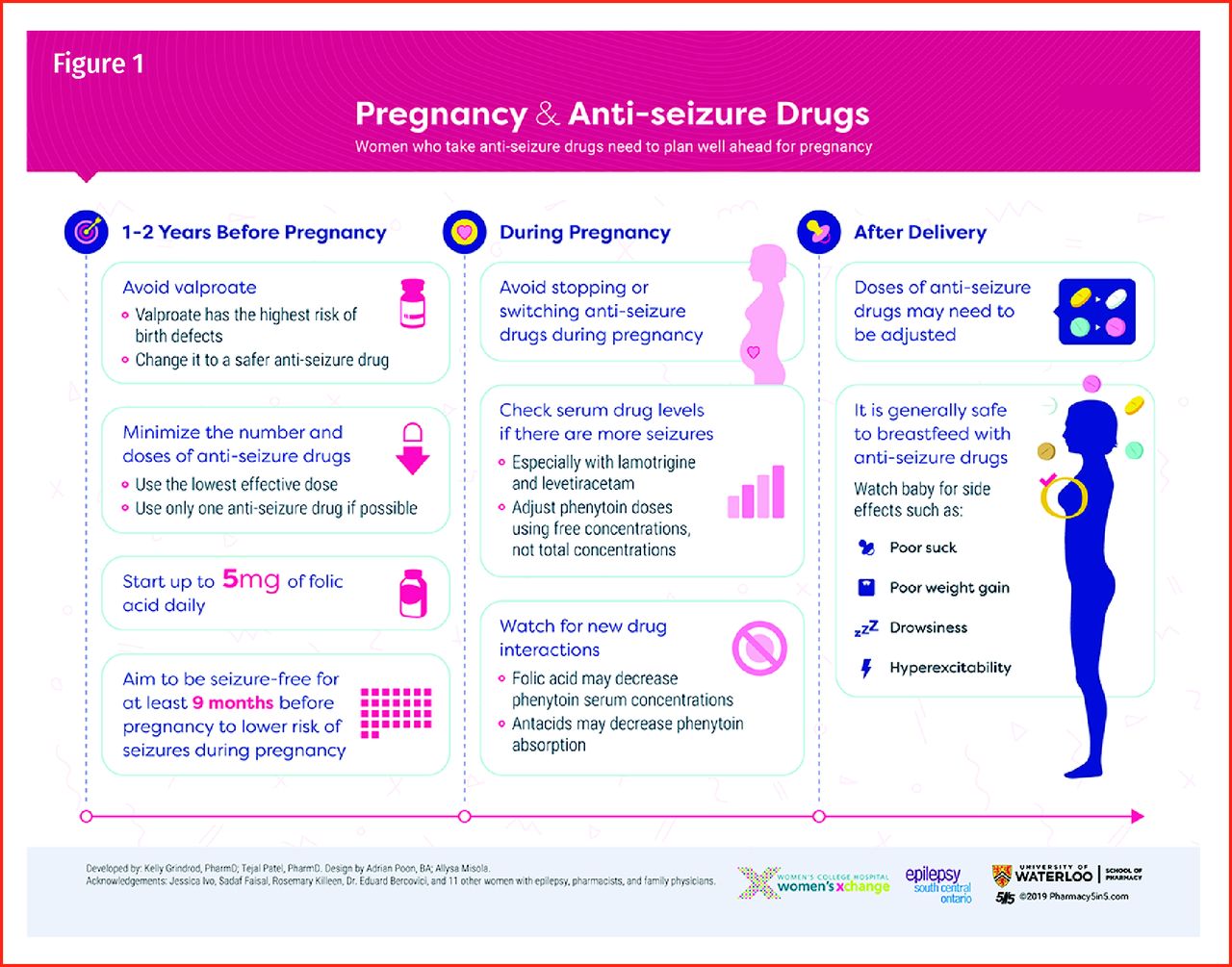
All women with epilepsy of childbearing age should receive preconception counseling and should be encouraged to start planning for a pregnancy at least 1 to 2 years in advance.2,5–8 First, women should be aware that all antiseizure drugs increase the risk of birth defects, and that valproate (valproic acid, divalproex acid) has the highest risk and should be avoided in pregnancy.9–11 The Ontario treatment guidelines can be useful for choosing safer alternatives for different seizure types or epilepsy syndromes.11 Second, the risk of teratogenicity with antiseizure drugs is dose related,12 and each drug carries its own risks. Where possible, women with epilepsy who are planning for a pregnancy should take the fewest number of drugs at the lowest effective doses needed for seizure control. Third, they should aim to be seizure free for at least 9 months before pregnancy, as this increases the likelihood they will remain seizure free during pregnancy.13 Finally, many antiseizure drugs affect folic acid levels, and planning ahead allows women to start folic acid supplementation. Use folic acid doses of at least 0.4 mg daily, or up to 5 mg daily for women who have a higher risk of offspring with neural tube defects or to reduce the risk of cognitive effects in the offspring from antiseizure drugs.2,3,7,11 Thus, a woman who takes valproate for seizures, for example, should be aware that if she wishes to become pregnant, she will need time to taper the valproic acid, start a safer alternative, optimize the dose for seizure control, be seizure free for at least 9 months before pregnancy, and start taking folic acid.
During pregnancy, antiseizure drugs should not be stopped or switched, as that can lead to poor seizure control. As the risk of teratogenicity increases with dose, doses should also be increased cautiously. That said, antiseizure drug doses might occasionally need to be adjusted in response to the physiological changes of pregnancy.2,3,7 For example, the serum concentrations of levetiracetam and lamotrigine will often decline during pregnancy. Women who experience seizures when serum drug concentrations fall might need a higher drug dose. Women who have complete seizure control despite a drop in their serum drug concentration do not necessarily need a higher dose. Doses adjusted during pregnancy might also need to be decreased again after the baby is born.3 Of note, while the total concentration of phenytoin might also decline, the free phenytoin concentration is a more useful measure, as it often remains unchanged. As with other drugs, if a woman experiences seizures when the free phenytoin concentration falls, she might need a higher dose.
Finally, most antiseizure drugs are considered to be safe or moderately safe for breastfeeding, although ethosuximide is contraindicated.14 Clinicians should advise women who breastfeed while taking antiseizure drugs to monitor for signs of toxicity in infants, such as abnormal muscle tone, poor feeding and growth, or sedation.14
Antiseizure drugs and birth control
Copper intrauterine devices (IUDs) and levonorgestrel IUDs are the only 2 forms of contraception that are unaffected by antiseizure drugs. Many antiseizure drugs are potent inducers of the cytochrome P450 enzymes, meaning they increase the number of metabolizing enzymes in the liver.2,3,15–17 Estrogen (and progesterone to a lesser extent) is primarily metabolized by cytochrome P450 3A4 enzymes, although 2C9, 2C19, and 3A5 might also play a role. As a result, when oral combined hormonal contraceptives are taken together with an enzyme inducer such as carbamazepine or phenytoin, the increased first-pass hepatic metabolism lowers the estrogen serum concentrations and increases the risk of unplanned pregnancy. Women who take oral combined hormonal contraceptives should use a product with at least 30 µg of ethinyl estradiol. While some authors recommend using at least 50 µg of ethinyl estradiol,16,18 there are no products with this amount of ethinyl estradiol available in Canada. Women might also prefer tri-cycling or long-cycling, where a pill is taken daily with a pill-free interval of 4 to 7 days, every 3 months.18 Alternatively, women could choose medroxyprogesterone acetate intramuscular injections, which can be administered every 10 to 12 weeks.16 Women who opt for non-IUD hormonal contraception can also further decrease their risk of pregnancy by using a barrier method.
In contrast to the above interaction, estrogen can also increase the metabolism of lamotrigine and valproic acid.17 A woman who is seizure free while taking either lamotrigine or valproic acid might experience an increase in seizure frequency after starting an estrogen product. In these cases, the dose of valproate or lamotrigine can be increased as needed for the control of seizures.
Other considerations
The interaction between estrogen and antiseizure drugs also has implications beyond the childbearing years. For example, women who use estrogen for menopausal hot flashes might need higher doses if they use an enzyme-inducing antiseizure drug. Similarly, women who have used antiseizure drugs for many years have a higher risk of osteoporotic fractures, both due to falls from seizures and to the effects antiseizure drugs on bone health.4 All women who take antiseizure drugs should ensure they get enough calcium, vitamin D, and exercise. Finally, many women take antiseizure drugs for various indications including chronic pain, mood, and headache. These women face will similar challenges to those faced by women with epilepsy.
Conclusion
There are many special considerations for women who use antiseizure drugs, regardless of the indication. Clinicians should ensure that they take the time to educate all women who use these drugs on the effects the drugs can have on contraception, pregnancy, breastfeeding, and hormones later in life.
Acknowledgments
We thank Adrian Poon for designing the infographic, and Jessica Ivo, Sadaf Faisal, Rosemary Killeen, Dr Eduard Bercovici, and the women with epilepsy, pharmacists, family physicians, and neurologists who reviewed it. This work was funded through a grant from the Women’s Xchange through Women’s College Hospital in Toronto, Ont.
Notes
We encourage readers to share some of their practice experience: the neat little tricks that solve difficult clinical situations. Praxis articles can be submitted online at http://mc.manuscriptcentral.com/cfp or through the CFP website (www.cfp.ca) under “Authors and Reviewers.”
Footnotes
↵* The infographics on use of antiseizure drugs in pregnancy and breastfeeding (Figure 1) and antiseizure drug interactions with hormonal contraception (Figure 2) are available at www.cfp.ca. Go to the full text of the article online and click on the CFPlus tab.
Competing interests
None declared
- Copyright© the College of Family Physicians of Canada
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.