


Many decisions in health care (diagnosis, treatment, screening, etc) warrant shared decision making (SDM); however, this approach has not yet been sufficiently integrated in clinical settings.1 Some clinicians might think this process is not relevant, might doubt the ability of patients to make decisions, do not feel they have the capacity to share information in an appropriate format, or have misconceptions about what SDM involves.2 A common barrier evoked by physicians is the additional time required, even though the literature suggests SDM adds only a few extra minutes to the consultation time (median of 2.6 minutes).3 Still, as time is precious, we need to reflect on when SDM is warranted and when it is not.
What is SDM?
Shared decision making “is not about convincing the patient to follow the doctor’s recommendation. Nor is it about ... leaving your patient to decide on his or her own.”4 It recognizes patient self-determination as an important piece of the doctor-patient relationship. It is different from a motivational interview and is more than simply sharing information.
Shared decision making is “an approach where clinicians and patients share the best available evidence when faced with the task of making decisions, and where patients are supported to consider options, to achieve informed preferences.”5 Elwyn and colleagues proposed a 3-step model for SDM that can be summarized in 3 specific actions (Figure 1).5 This model describes SDM as a deliberation process that respects what matters most to patients.

For SDM to be useful, there must be a clear need for a decision. For a decision to warrant SDM, there should be different options with a balance of benefits and harms (a certain equipoise) to address the issue at hand. The premise of SDM is to recognize (patient and clinician alike) that there are often many reasonable medically valid options, each with potential benefits and harms, and that the optimal decision might be very different from one person to the next depending on their life circumstances, values, and preferences.
Shared decision making has many benefits such as increased patient and physician satisfaction, increased patient knowledge, and reduced decisional regret.3 It is increasingly seen as an ethical imperative; however, training and continuing education opportunities in SDM are still lacking.
While SDM is mostly underused, at times it is introduced in situations when it probably should not be. For example, it is introduced when there is no decision to be made; when the patient cannot collaborate in the process; or when, on balance, estimates of benefits versus harms of a test or treatment do not justify such an approach. This article highlights these situations and discusses some limitations of SDM. In so doing, we aim to help clinicians better focus their time and energy on situations where SDM can really make a difference.
Case description
You recently attended a conference about SDM and realized that you should try to incorporate it in your practice. Although you were told this will not increase your visit time with your patients, you are sceptical. You are wondering how to choose when to use SDM or not. Shared decision making is a tool, like your stethoscope, so surely there are times when it is helpful and other times when it is not. For example, a patient with respiratory symptoms of viral origin (eg, acute bronchitis) might need information but does not require SDM about whether to start an antibiotic. In contrast, a depressed patient will likely benefit from SDM when deciding between 2 reasonable options (eg, antidepressants or psychotherapy).
It might look like SDM, but …
The bronchitis example above reflects a situation with only 1 valid therapeutic option—namely managing symptoms until they disappear on their own. Shared decision making helps patients weigh the benefits and harms of different options that offer a somewhat similar benefit-to-harm ratio. It does not mean that we need to present every option including those that cannot deliver a reasonable chance of benefit but might cause harm.
Another example is using a decision aid about cancer screening with patients with multiple comorbid conditions. The reduced life expectancy of these patients likely precludes any benefit from the proposed intervention. The use of SDM about mammography screening for a frail 70-year-old woman might be perceived as an ethical dilemma. Some would say she is entitled to the information; but in this patient any benefit is unlikely. On the other hand, more immediate harms are quite possible; so, this decision cannot be in equipoise. Readers of this series might remember a similar example offered in another article.6
A third example is exploratory laparotomy for chronic persistent functional abdominal pain in a young otherwise healthy person. This option does not need to be discussed with these patients.
When is SDM warranted?
As time is precious, discerning when SDM is appropriate and likely to make a difference in care is important. There are certain circumstances in which SDM is not used enough and in which it would be a worthwhile time investment. Recognizing that some decisions do not need to be rushed (for example, screening for lung cancer), you can decide to interact immediately with the patient or postpone the conversation until the patient has had a chance to learn more about the decision (possibly with a decision aid).
In many instances, there are multiple options, each with its pros and cons, and instead of offering an opinion, a shared decision is often more beneficial. Hot flashes from menopause have different treatment options. The decision about which option to pursue is influenced by values and preferences, and thus should be shared. If no decision aid exists, a generic tool like the Ottawa Personal Decision Guide7 can be helpful. It provides a structured tool for the patient and physician to list options and it guides patients in their reflection.
There are many other examples, as a substantial proportion of care is considered to be preference sensitive.8 For example, which medication should follow metformin in the treatment of type 2 diabetes, which medication should be prescribed first in depression, or whether a medication should be used to lower cholesterol or prevent fragility fractures.9
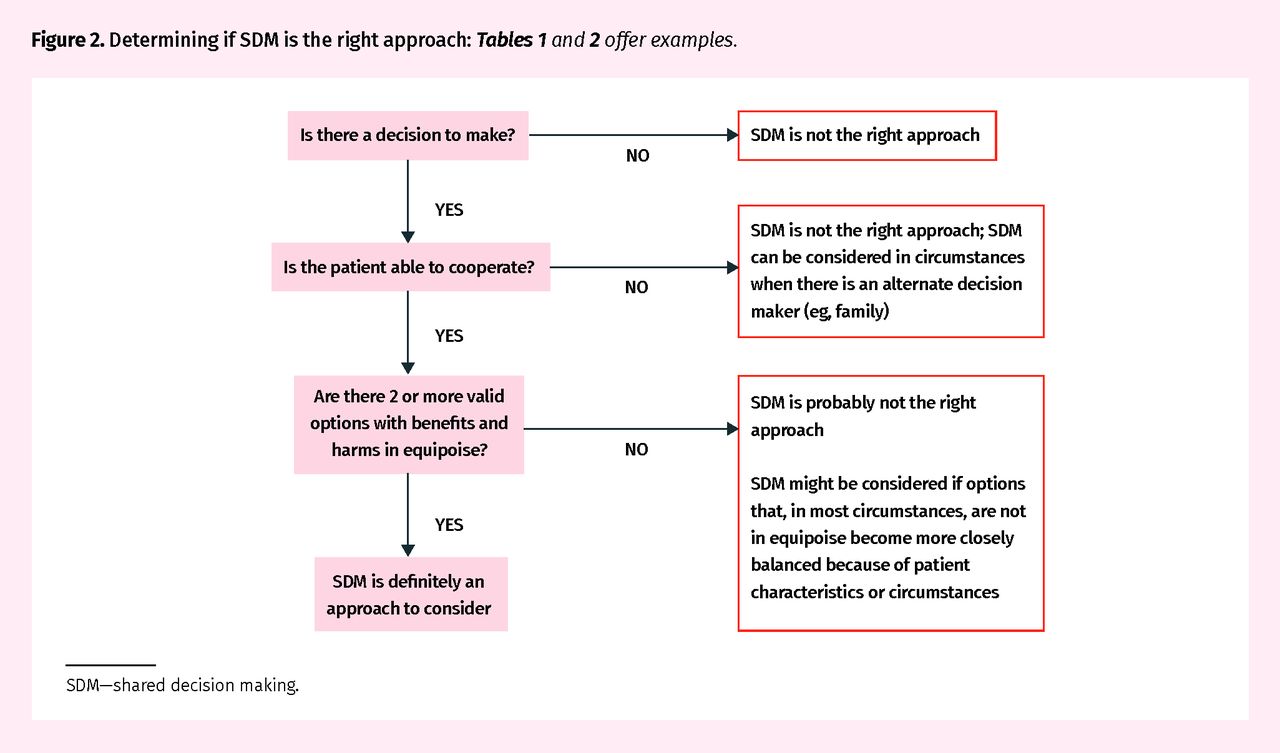
There is a continuum of when it might be appropriate to use SDM. That does not mean we should not try to reflect on when SDM is warranted or not. Tables 1 and 2 provide some thinking points.10–19 The examples are not meant to be prescriptive, but to foster clinicians’ reflections about the place of SDM in their practice. Figure 2 illustrates an algorithm for determining if SDM is the right approach.

Determining if SDM is the right approach: Tables 1 and 2 offer examples.
SDM—shared decision making.
When SDM should be considered
When SDM should probably not be considered
Limits of SDM
There are many medical circumstances in which SDM is warranted but, even though we think there is a balance between benefits and harms, no quantitative information about the different alternatives is available. In these instances, we have to accept this fact and share the uncertainties.
Imagine you have a 26-year-old woman with repeated blood pressure measurements equal to or just above 140/90 mm Hg. You would like to share the benefits and harms of treatment; however, we know of no reliable way to estimate her future risk of cardiovascular disease or to compare the potential benefit of nondrug with drug therapy at this age. Any clinician who truly embraces SDM will, at times, be confronted with situations like these. Shared decision making can sometimes be facilitated with decision aids20 but need not be limited to situations for which a decision aid exists.
The patient has to remain central to the decision
Imagine a 64-year-old patient with severe chronic obstructive pulmonary disease who asks about colon cancer screening. The Canadian Task Force on Preventive Health Care recommends screening adults 60 to 74 years of age for colorectal cancer (strong recommendation), but given the severe chronic obstructive pulmonary disease, the situation needs a different approach, as the likelihood of benefiting from this screening is so low compared with the potential risk of harm. Information and support, more than SDM, is likely the right approach here.
In a recent article in this series,6 we debated the opposite situation. Namely, at times, even for recommendations against screening maneuvers, benefits might surpass the potential harms—for example in elderly but fit individuals. The Canadian Task Force recommendation on colon cancer screening in adults aged 75 and older is a weak recommendation against screening. This is based on low-quality evidence and a generally reduced life expectancy in this age group. Still, some adults older than 75 years without serious comorbidities might decide to continue screening. The decision comes down to values and preferences and knowing about the median life expectancy of Canadians at an advanced age. There will always be gray zones, and that is why you should gather information about your patient before deciding if SDM is a good approach.
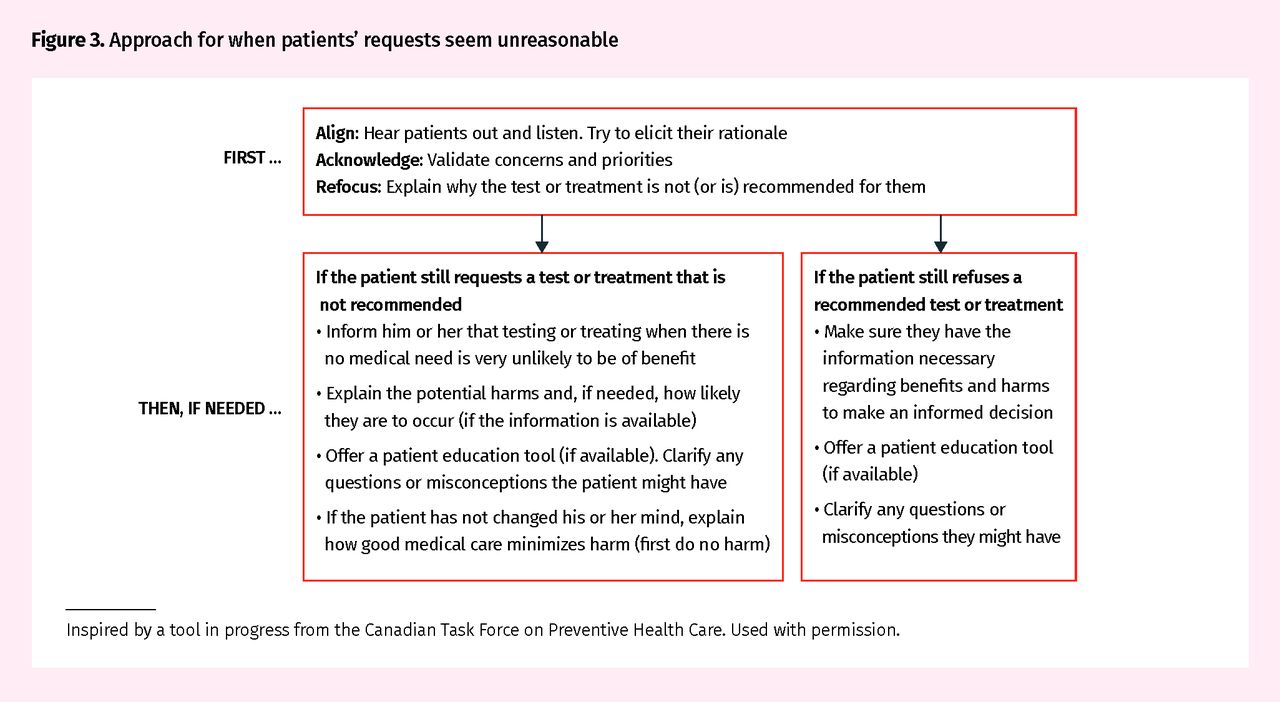
Patients we feel make unreasonable requests
Some patients want a test or treatment where the recommendation is strongly against it or will refuse an intervention where the benefits clearly seem to outweigh the harms. Communicating in such circumstances is outside the realm of SDM because the options are not in equipoise. However, we can suggest an approach that can be useful. For example, if you encounter a 78-year-old man who wants a prostate-specific antigen test to screen for prostate cancer, you could simply state this is not a good idea. But what if the patient insists? What if you have an asymptomatic patient who wants thyroid-stimulating hormone screening? A patient with acute low back pain requesting magnetic resonance imaging? A 40-year-old woman who refuses a Papanicolaou test? A patient with elevated blood pressure who refuses treatment? A patient with diabetes who refuses an eye examination or medications to control diabetes? One strategy is to “align, acknowledge, and refocus” (Figure 3).
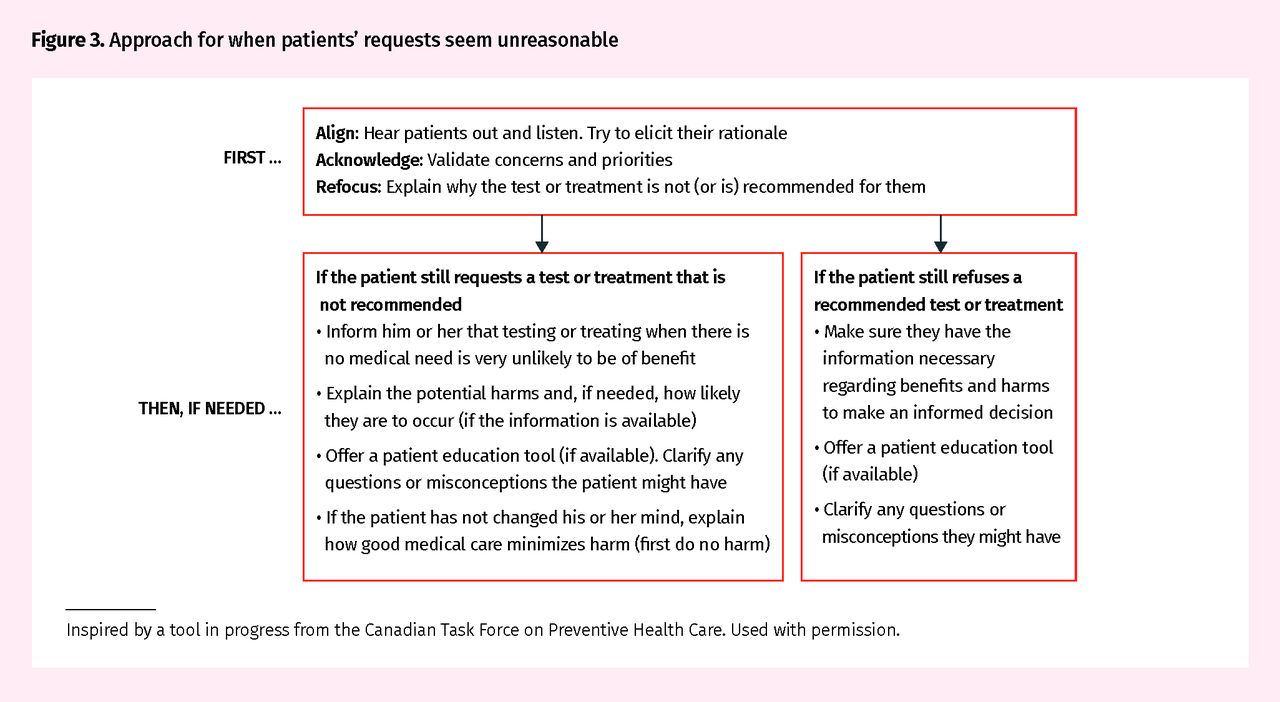
Approach for when patients’ requests seem unreasonable
Inspired by a tool in progress from the Canadian Task Force on Preventive Health Care. Used with permission.
Patients who want health professionals to decide for them
It is a widespread myth that all patients want physicians to make decisions for them. Even if a certain percentage of patients would prefer the doctor to make the decision, this is not a reason to avoid SDM altogether. Most patients appreciate SDM, while a small percentage prefer to make the decision alone.21 The physician might be the expert in the disease, but remember that the patient is the expert on living with the disease (or the consequences of an action).
Case resolution
You have now reflected on what SDM is and what it is not, when it is worthwhile and when it is not. You recognize that there are times we should do it and times when we do not need to. You realize that you were not using this approach in discussions about screening, and that is a place where many conditional recommendations warrant such an approach.
As knowledge translation tools for screening decisions are readily available,22 you decide that introducing SDM for these will be a good first step. You will use these tools before ordering a woman’s first mammogram or if a patient asks about prostate cancer screening.23 You will also ensure you have information pamphlets for situations in which SDM is not warranted (eg, bronchitis, acute low back pain).24,25
Once you feel comfortable with the approach, you intend to use decision aids for common therapeutic decisions, like choices about diabetes medication or antidepressants. You feel these will be easy to implement and will make sure to share this approach with your colleagues. You also intend to reflect on how this change in practice could be evaluated to capture improvements in outcomes that matter.26
Notes
Key points
▸ While shared decision making (SDM) is often underused, it is sometimes introduced in situations when it probably should not be.
▸ Generally, SDM should be considered when there are at least 2 medically valid options, each with a balance between benefits and harms (equipoise).
▸ When SDM is not warranted, sharing information remains a good practice.
Footnotes
Competing interests
All authors have completed the International Committee of Medical Journal Editors’ Unified Competing Interest form (available on request from the corresponding author). Dr Singh reports grants from Merck Canada, personal fees from Pendopharm, and personal fees from Ferring Canada, outside the submitted work. The other authors declare that they have no competing interests.
This article is eligible for Mainpro+ certified Self-Learning credits. To earn credits, go to www.cfp.ca and click on the Mainpro+ link.
La traduction en français de cet article se trouve à www.cfp.ca dans la table des matières du numéro de mai 2020 à la page e149.
- Copyright© the College of Family Physicians of Canada
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- The paradox of using SDM for de-implementation of low-value care in the clinical encounter
- Reduire les dosages systematiques inutiles de la vitamine D
- Reduce unnecessary routine vitamin D testing
- Depistage en prevention primaire des fractures de fragilisation: Combien de temps faut-il?
- Screening for primary prevention of fragility fractures: How much time does it take?
- The limits of shared decision making
- The paradox of using SDM for de-implementation of low-value care in the clinical encounter
- Patient decision aid for flozins in heart failure and ejection fraction greater than 40%
- Aide a la decision dutiliser ou non les gliflozines pour linsuffisance cardiaque avec fraction dejection superieure a 40 %, a lintention des patients
- Que devraient enseigner les educateurs pour ameliorer les soins de sante preventifs?
- What should educators teach to improve preventive health care?
- Going against the status quo in screening: Call to action to improve teaching in preventive health care
- A lencontre du statu quo en matiere de depistage: Appel a laction pour ameliorer lenseignement des soins de sante preventifs
- Equipoise is preference sensitive