


Varicella-zoster virus (VZV) infection causes primary varicella (PV; ie, chickenpox). Infection by VZV is lifelong; after primary infection, it lies latent in the dorsal root ganglia until reactivation, where it results in herpes zoster (HZ; ie, shingles). Varicella-zoster virus is present worldwide and 98% of the adult population in the United States is seropositive for VZV.1 In Canada, implementation of varicella immunization programs across the country has resulted in a 99% decline in average incidence of varicella.2
Although PV is often regarded as a disease of childhood, it can also present in unvaccinated adults or adults with waning immunity. In healthy individuals, PV is often a benign disease mostly limited to cutaneous involvement.3 However, in high-risk individuals, like those who are immunodeficient or pregnant, PV can disseminate to visceral organs such as the liver or lungs. Primary varicella in adults tends to be more severe, and healthy adults might develop complications from varicella.4 We report the case of a 90-year-old man who presented to the emergency department with disseminated PV.
Case
A 90-year-old man presented to the emergency department with a 2-day history of fever, malaise, nausea, and diffuse pruritic cutaneous eruption on his head and neck. The eruption progressed inferiorly toward his distal extremities and new vesicles formed centrally within pre-existing erythematous macules. He denied sick contacts or recent travel but recalled spending time with his newborn great-grandchild 2 weeks previously. The patient’s past medical history included metastatic gastrointestinal stromal tumours. The patient had seen his family physician 2 days previously with constitutional symptoms and was prescribed cephalexin empirically for a suspected urinary tract infection. Upon physical examination, the patient was afebrile, with unremarkable vital signs. An examination of his skin revealed multiple clear vesicles on erythematous macules distributed all over his body, suggesting “a dewdrop on a rose petal” appearance (Figures 1 and 2). He was disoriented to time. Further examination findings were unremarkable. Bloodwork revealed a 5-fold increase in transaminase levels and a 75% increase in creatinine level from baseline, suggesting acute hepatic dysfunction and acute-on-chronic kidney injury. Dermatology, internal medicine, infectious disease, and medical oncology departments were all consulted. Cephalexin drug eruption was the postulated diagnosis; however, a second dermatologist reviewed the presentation and diagnosed PV based on the classic clinical appearance. Intravenous acyclovir was initiated for suspected VZV encephalitis. Skin biopsy findings demonstrated necrotic keratinocytes with prominent herpetic intranuclear inclusions. Results from viral polymerase chain reaction testing of a skin swab from a vesicle confirmed VZV and were negative for herpes simplex virus (HSV) types 1 and 2. The patient was placed in airborne isolation during his hospital admission and was discharged only after all the lesions had crusted.

The patient presented with generalized erythematous papules and vesicles in various stages of healing

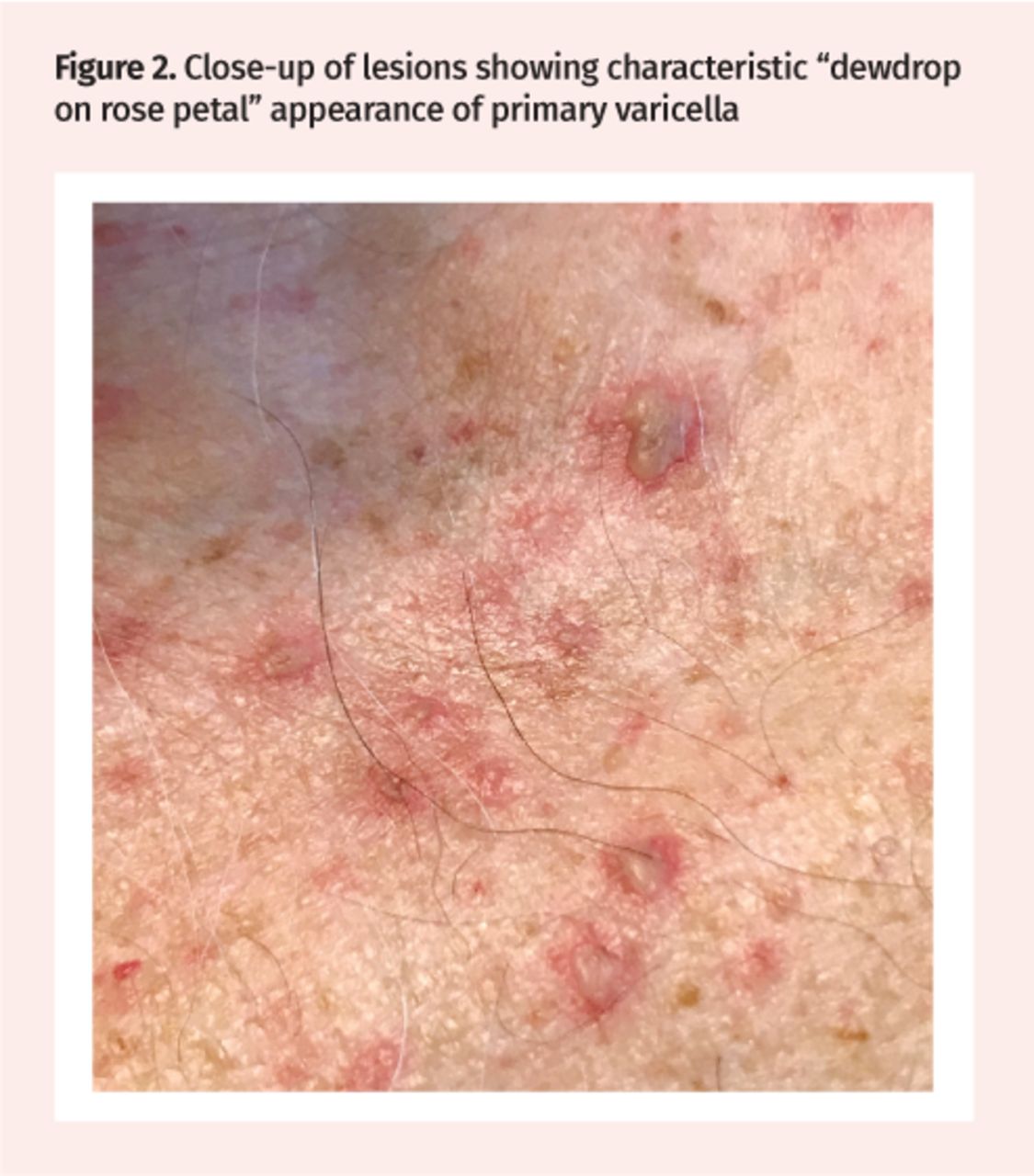
Close-up of lesions showing characteristic “dewdrop on rose petal” appearance of primary varicella
Discussion
PubMed and MEDLINE searches were completed using the 2 MeSH terms chickenpox and varicella zoster virus infection, with preference given to review articles published after 1995. Article references were hand searched for relevant publications.
The incidence of PV in Canada has declined substantially with implementation of routine varicella vaccination programs in the pediatric population across provinces and territories between 2000 and 2007.2 Annual incidence of PV has declined from 214.3 cases per 100 000 before the vaccine to 3.1 cases per 100 000 between 2011 and 2015.2 Children benefit from protection rates of 94.4% and 98.3% following a single dose and a second dose of varicella vaccine, respectively.5 This decline in PV incidence has resulted in decreased suspicion and detection rates among clinicians.6
Varicella-zoster virus is highly contagious and is transmitted through airborne droplets or direct contact with vesicular fluid.4 Transmission of VZV can occur from either PV or HZ. The affected individual is infectious beginning from 2 days before the onset of rash and remains infectious until all vesicles have crusted (typically 5 days after rash onset).4 The incubation period of VZV is 10 to 21 days.7
A family physician’s office is often the first place that patients will visit when ill, hence it is important that family physicians recognize PV early on to prevent transmission to other patients. Nosocomial transmission of VZV is primarily airborne.8 Early recognition is not only crucial to prevent transmission but also to prevent potentially life-threatening effects on others, such as pregnant women and their fetuses. Mortality rates from PV are higher in pregnant women than nonpregnant women, and potential maternal complications include respiratory pneumonitis.9 Fetal complications can include birth malformations from congenital varicella syndrome or multiorgan failure in neonates, especially if PV infection occurs during gestational weeks 13 to 20.5
Primary varicella presents with discrete pruritic papules and vesicles in different evolutionary stages, with the classic description “dewdrop on a rose petal.”10 The rash typically starts on the head and neck before spreading to the trunk and extremities in a cephalocaudal progression. Younger clinicians might be unfamiliar with the presentation of PV, as its incidence has declined.6,11 Primary varicella is usually seen in susceptible unvaccinated individuals, but can also present in individuals who had been previously vaccinated, which is referred to as “breakthrough varicella.”12 In otherwise healthy children, PV is relatively benign, mainly limited to cutaneous involvement.4 However, infection from PV in healthy adults can result in more severe disease and higher rates of complications.4 In high-risk populations, such as immunodeficient or pregnant individuals, PV can disseminate and involve multiple organ systems.4 Disseminated PV is associated with high morbidity and mortality, with complications including myocarditis, gangrene, hepatitis, and glomerulonephritis.13 Hepatitis and glomerulonephritis likely occurred in this patient.
The differential diagnosis in this patient includes disseminated HSV or disseminated HZ. Disseminated HSV typically presents with painful, grouped vesicles on a confluent erythematous base. Primary varicella and disseminated HSV histopathology findings from a skin biopsy can look identical, hence viral polymerase chain reaction of vesicular fluid is necessary to differentiate the 2 viruses.14 Herpes zoster typically presents with grouped vesicles in a unilateral, dermatomal distribution. Disseminated HZ can involve multiple dermatomes and can be bilateral. However, dermatomal involvement remains visible and will aid diagnosis. While hepatic dysfunction alone can occur in adults with PV, the concomitant presentation of acute-on-chronic kidney disease, fluctuating level of consciousness, and hepatic dysfunction in the patient presented in this case suggests disseminated PV. A lumbar puncture and cerebral magnetic resonance imaging were contraindicated owing to the patient’s pacemaker and overlying rash on the spine.
For susceptible individuals who are healthy, nonpregnant, and older than 12 months of age, the varicella vaccine can be administered up to 5 days after exposure to prevent or reduce the severity of PV.5 For nonimmune individuals who are ineligible to receive the varicella vaccine, such as infants, pregnant women, or immunocompromised individuals, an alternative post-exposure treatment is varicella zoster immune globulin.5 If varicella zoster immune globulin is unsuccessful at preventing PV, it might still reduce the disease severity if given within 10 days after exposure.5 Varicella zoster immune globulin is most efficacious if given within 4 days after exposure.5
Acyclovir is the first-line treatment option for PV to prevent disease progression, prevent complications, and hasten recovery. Acyclovir is typically used in the high-risk populations described,15 but acyclovir use in immunocompetent children has been shown to result in a shorter duration of disease, fewer skin lesions, and accelerated lesion healing.16 Acyclovir should be considered in all individuals regardless of immune status or disease severity.17
Conclusion
This case demonstrates how multiple physicians from various specialties were unable to recognize a case of PV with classic presentation. With a decline in PV incidence, it is possible that PV presentation is now so uncommon in clinical practice that it is more difficult to identify. Complications of PV can present in pregnant women, immunodeficient individuals, or in healthy adults. Advanced age can be a barrier to diagnosis, as PV is often regarded as a disease of childhood. A delay in PV diagnosis can lead to substantial morbidity and mortality, especially in high-risk individuals. Early recognition of PV is also important to prevent transmission to others, especially to those at increased risk of complications, including susceptible adults, susceptible pregnant women, susceptible immunocompromised individuals, and fetuses of nonimmune pregnant women.
Notes
Editor’s key points
▸ Primary varicella (PV) appears as discrete pruritic papules and vesicles in a “dewdrop on a rose petal” pattern. With the decline in PV incidence, it is possible that PV presentation is now so uncommon in clinical practice that it is difficult to identify.
▸ As PV and herpes simplex virus histopathology findings from a skin biopsy can look the same, polymerase chain reaction of vesicular fluid is needed to differentiate between the viruses.
▸ Advanced age can be a barrier to diagnosis, as PV is often regarded as a disease of childhood. A delay in PV diagnosis can lead to substantial morbidity and mortality, especially in high-risk individuals. Early recognition of PV is also important to prevent transmission to others, especially to those at increased risk of complications, including susceptible adults, susceptible pregnant women, susceptible immunocompromised individuals, and fetuses of nonimmune pregnant women.
Points de repère du rédacteur
▸ La varicelle primaire (VP) apparaît sous forme de papules et de vésicules prurigineuses, disposées comme une « goutte de rosée sur un pétale de rose ». Compte tenu du déclin dans l’incidence de la VP, il est possible que la présentation de la VP soit maintenant si rare en pratique clinique qu’elle soit difficile à reconnaître.
▸ Parce que les constatations d’une histopathologie de dépistage de la VP et du virus de l’herpès simplex à la suite d’une biopsie de la peau se ressemblent, il est nécessaire de procéder à une amplification en chaîne par polymérase du fluide vésiculaire pour faire la distinction entre les 2 virus.
▸ L’âge avancé peut compliquer le diagnostic puisque la VP est souvent considérée comme une maladie infantile. Un retard dans le diagnostic peut entraîner une morbidité et une mortalité considérables, surtout chez les personnes à risque élevé. Il est aussi important de reconnaître rapidement la VP pour prévenir la transmission à d’autres personnes, surtout celles à risque élevé de complications, notamment les adultes vulnérables, les femmes enceintes vulnérables, les personnes immunodéprimées vulnérables et les fœtus de femmes enceintes non immunisées.
Footnotes
Competing interests
None declared
This article has been peer reviewed.
Cet article a fait l’objet d’une révision par des pairs.
- Copyright© the College of Family Physicians of Canada
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.