


Abstract
Objective To present a case-based discussion on the workup of male factor infertility and review currently available treatments.
Sources of information This discussion is based on the current Canadian Urological Association and American Urological Association guidelines, with reference to landmark papers as appropriate from 2010 onward. All articles were retrieved through PubMed.
Main message Approximately 15% of Canadian couples experience infertility, making it a commonly encountered condition in the primary care setting. Among couples suffering from infertility, male factors can be identified as the sole cause in 30% of cases and as a contributing issue in 20% of cases. Although many of the treatments described aim to improve a couple’s chances of naturally conceiving a child via intercourse, many patients ultimately require medical or surgical intervention to achieve pregnancy. This can be a long, protracted course for patients, with important roles for primary care providers and fertility specialists alike.
Conclusion Male fertility assessment and treatment has historically been left in the hands of fertility specialists, creating a bottleneck for patients to receive fertility care. However, with increased understanding of the underlying causes of male factor infertility, the workup and initial management can occur in the primary care setting, helping to streamline care.
Infertility affects 15% of couples in Canada, and is defined as failure of a couple to become pregnant within 1 year of regular unprotected intercourse.1 Regular intercourse is defined as intercourse every 2 to 3 days. Male factors are identified as the sole cause in 30% of cases, female factors are identified as the sole factor in 35% of cases, 20% of cases have a combination of female and male factors, and 15% have no identifiable cause.2
Despite this being a relatively common problem, training on male fertility is largely limited to urologists, often those who have undergone subspeciality fellowship training in this domain. However, the initial workup and diagnosis of men with fertility issues can be completed by primary care physicians, helping to streamline care and alleviate the accompanying stress and anxiety among couples struggling to conceive.
This review presents the foundational definitions of male factor infertility, the initial workup of this condition, and the medical and surgical options currently at urologists’ disposal for treatment of common conditions affecting male fertility.
Sources of information
This case-based discussion on male infertility is based on the current Canadian Urological Association1 and American Urological Association3 guidelines on this subject, with reference to landmark papers as appropriate from 2010 onward. All articles were retrieved through PubMed.
Case description
A 35-year-old man, whose partner is a 32-year-old woman, presents with difficulty to conceive for 1 year. What is the diagnostic workup?
Main message
Definitions of abnormal semen analysis findings. By far the most common test ordered for men with suspected infertility is semen analysis. For ordering providers, it is important to understand the different results one might encounter, as they affect subsequent diagnostic testing and treatment choices. Although there are many types of abnormal findings (Table 1),4 the most common include those associated with low sperm counts.5 This can include men with azoospermia (0 sperm noted on analysis) or oligospermia (less than 15 million sperm noted on analysis).
Definitions of common abnormalities noted on semen analysis
The diagnostic workup of men presenting with suspected infertility includes performing an in-depth history and focused physical examination. The male fertility history is one of the most comprehensive histories performed in the field of urology, focusing on the many identified risk factors (Box 1).1,6 This history is largely focused on 2 aspects of male physiology: the hypothalamic-pituitary-gonadal (HPG) axis, and normal testicular development and function (Box 2). By identifying either inherited conditions or acquired insults to these 2 pathways, clinicians can focus their diagnostic tests or treatments to improve a patient’s fertility potential. Similarly, a focused physical examination can help identify potentially reversible findings (eg, varicocele) that patients might not have been previously aware of.
Review of focused male infertility history and physical examination
Focused male fertility history
Infertility history: duration, primary or secondary, sexual function and activity, lubricant use
General health: diabetes, recent severe illness or infection, history of respiratory illness
History of any genitourinary infections, testicular infections, or trauma to scrotum or pelvis
Any surgery of reproductive tract including testicular cancer, hydrocelectomy or spermatocelectomy, vasectomy, varicocelectomy, or inguinal hernia surgery
Review of current and recent medication use: steroid therapy, antibiotic use, chemotherapy, narcotics
Environmental exposures: pesticides, exposure of testicles to heat
Review of drug and alcohol use
Review of any genetic abnormalities and infertility history noted in family
Focused male fertility physical examination
Virilization state, body habitus, gynecomastia
Scrotal examination: presence of varicocele, presence of vas deferens, size and consistency of testicles and epididymis
Abdominal examination: inguinal scars (possible cryptorchidism repair or inguinal hernia repair), other abdominal scars, radiation tattoo markers
Special circumstances: sense of smell (Kallmann syndrome), chest examination for situs inversus (Kartagener syndrome), visual fields (pituitary prolactinoma)
Review of common risk factors for male infertility
Common risk factors for male infertility include the following:
Patient factors: age, history of testicular torsion
Congenital conditions: sickle cell disease, cryptorchidism, cystic fibrosis, hemochromatosis, Klinefelter syndrome, Kallmann syndrome
Lifestyle: obesity, stress, alcohol use disorder, cigarette smoking, marijuana smoking, illicit drug use
Medical conditions: diabetes, chronic kidney disease
Medications: testosterone therapy, steroids, α-blockers, antiandrogens, and many others with more subtle effects
Infections: orchitis, urethritis, mumps, prostatitis, sepsis
Cancers: testicular cancer, history of chemotherapy or radiotherapy
With the history and physical examination complete, the next step is to perform the initial diagnostic evaluations. Based on available urologic male infertility guidelines, investigations typically begin with completing 2 properly collected semen sample analyses.1,3 For patients providing a semen sample at home, proper collection includes deposition of all seminal fluid into a specimen jar, keeping the specimen jar warm on the way to the laboratory (patients can be advised to place the sample in a shirt pocket), and delivering it to the laboratory within 1 hour. If the sperm concentration is less than 10 million sperm per millilitre, then a serum hormone profile might be of benefit to test the HPG axis.7 This is best achieved through testing the patient’s morning total testosterone and luteinizing hormone (LH) follicle-stimulating hormone (FSH) prolactin levels, and estradiol testing should be considered.1 Abnormal results in these investigations should prompt referral to a fertility specialist.
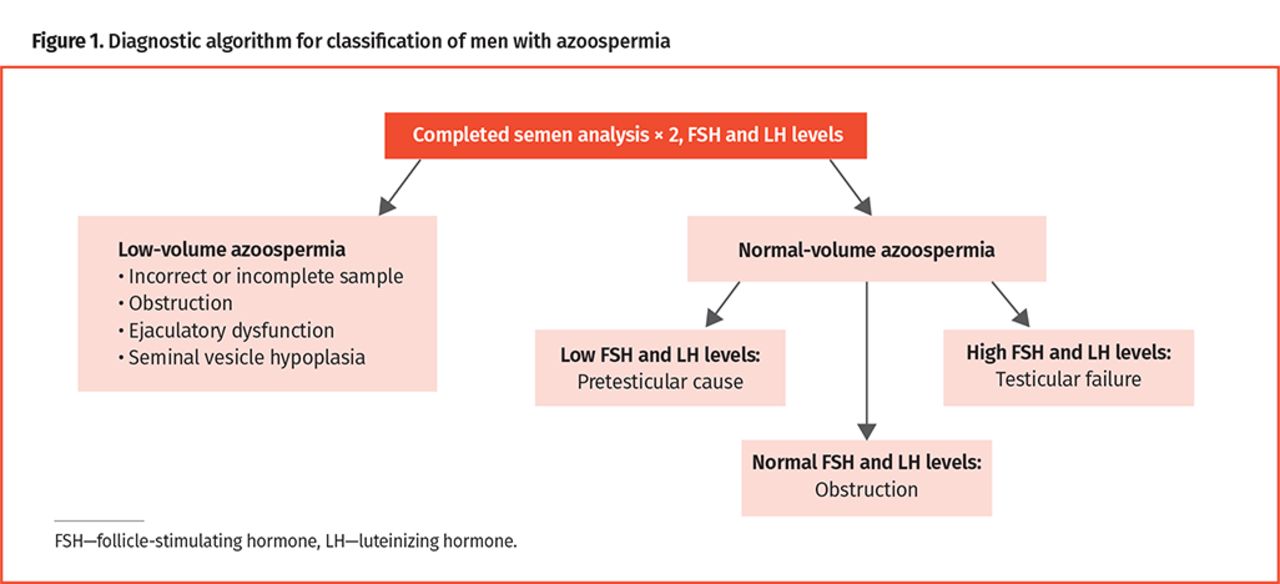
Findings of severe oligozoospermia or azoospermia should prompt a referral and most often require additional investigations by fertility specialists to diagnose the underlying cause. Assessment of semen volume allows classification of men with azoospermia into 1 of 2 categories: low-volume (semen sample less than 1.5 mL) or normal-volume azoospermia (Figure 1).

Diagnostic algorithm for classification of men with azoospermia
For those men with low-volume semen analysis findings, it must first be determined that collection and sample submission were performed correctly. If the low semen volume is confirmed, the man can then broadly be classified as having either obstructive azoospermia (typically accompanied by lower pH semen and absence of fructose) or an ejaculatory disorder such as retrograde ejaculation. Regardless of the cause, a postejaculatory urinalysis should be the first diagnostic step, with transrectal ultrasound being reserved for those with negative postejaculatory urinalysis findings. Performing transrectal ultrasound allows assessment for seminal vesicle dilation indicating ejaculatory duct obstruction. Men with low-volume azoospermia might also have absent vas deferens on physical examination, termed congenital bilateral absence of the vas deferens. Instances where one or both vas deferens are not palpable on physical examination should be followed by CFTR (cystic fibrosis transmembrane conductance regulator gene) testing for both the patient and the partner. If CFTR test results are negative, an abdominal ultrasound should be ordered to assess for other mesonephric duct abnormalities such as renal agenesis.
For men with normal-volume azoospermia, FSH levels allow for classification of men into broad categories of pretesticular (low FSH level), testicular (high FSH level), and posttesticular (normal FSH level) causes.
Most guidelines suggest that men with nonobstructive or indeterminate azoospermia or severe oligozoospermia (less than 5 million sperm/mL) should be offered genetic testing, with karyotype and Y microdeletion testing being the 2 most commonly performed tests.1,3 The completion of these tests typically require specialized laboratories.
Case update
The history of our patient is noncontributory, although he is noted to have small testicles bilaterally. He has no risk factors on review of history, and his partner has no fertility concerns. Findings of his semen analyses reveal normal-volume azoospermia. His FSH and LH levels are high, with a borderline low testosterone level. For now, you give him a presumptive diagnosis of nonobstructive azoospermia due to testicular failure. He requests information about possible treatments to achieve fertility and his chances of having a pregnancy with his partner.
What are the treatment options?
A comprehensive review of treatment options is presented below, although it should be noted that not all of the presented treatment options apply to the case presented.
Conservative treatment. With a thorough history, physical examination, and initial diagnostic tests completed, there is some advice that can be offered to all men dealing with infertility that might improve semen parameters and fertility.
Advising patients to optimize intercourse by having intercourse daily around partner ovulation and avoiding spermatotoxic lubricants is general advice all patients should receive. All men should be counseled to lead a healthy lifestyle, maintain a healthy body weight, and avoid alcohol and tobacco. All of these factors have previously been negatively associated with semen parameters.8 While conflicting studies exist, marijuana use, and certainly illicit drug use, should be stopped in men attempting to conceive with their partners.9,10 Clinicians should caution men from having prolonged exposure to heat (hot tubs, saunas, etc), although relatively few studies exist confirming a negative association with semen parameters.11
Nutritional supplements, multivitamins, and fertility supplements have gained widespread popularity in recent years, although data supporting these medications are largely lacking. Of the meta-analyses done on this topic, the only micronutrients or supplements that appear to show some benefit include selenium, l-carnitine, and coenzyme Q10, although even the authors of these analyses highlight that most studies included have substantial risk of bias and heterogeneity.12 No current male infertility guidelines recommend standardized use of nutritional supplements, and until further studies are completed, it is likely that clinicians cannot recommend any specific agent to their patients.1,3
Medical treatment. The hormonal manipulation of men’s HPG axis is likely best reserved for fertility specialists; however, an understanding of the currently available treatments is important given the increasingly prevalent use of these medications.
Selective estrogen receptor modulators (SERMs): Selective estrogen receptor modulators have been used for several decades to improve the hormonal profile of men, with the hopes of improving semen parameters and fertility as a result. These drugs work by blocking negative feedback of estrogen to the hypothalamus, allowing for increased levels of gonadotropins (specifically LH and FSH). However, well-controlled studies showing improved pregnancy rates have been lacking. A recent meta-analysis of the most common SERM used in male fertility, clomiphene citrate, showed a trend toward improved fertility, although no definitive conclusions could be drawn.13
Aromatase inhibitors: Aromatase inhibitors are another class of medications often used in men with infertility. These medications prevent the conversion of testosterone into estradiol, thereby acting to improve the hormonal profile of men and thus hopefully improve fertility. However, similar to SERMs, there are very few high-quality studies examining the benefits of this medication. The most recent systematic review on this topic failed to show any clear benefits of this medication class.14
Human chorionic gonadotropin: Human chorionic gonadotropin has been used with some effect in men with hypogonadotropic hypogonadism. In these men, a central (pituitary or hypothalamic) issue exists leading to poor or absent spermatogenesis. Restoration of a normal HPG axis can lead to a return of sperm to the ejaculate or improvement in semen parameters.15,16 Human chorionic gonadotropin can be given alone or in combination with exogenous FSH or human menopausal gonadotropin, allowing for a more physiologic hormonal supplementation.15
Testosterone: Although spermatogenesis largely relies on high intratesticular levels of testosterone, exogenous use of testosterone and anabolic steroids shuts down gonadotropin release through negative feedback at the pituitary gland and hypothalamus. Thus, exogenous testosterone will prevent both endogenous production of testosterone in the testicle and spermatogenesis. Patients potentially interested in family planning should not be offered testosterone therapy alone. A specialist referral should be considered to evaluate for reversible underlying causes of low testosterone. Another consideration is alternative therapies that preserve spermatogenesis, such as aromatase inhibitors and SERMs, or a combination of human chorionic gonadotropin and testosterone therapy.17 For patients using exogenous testosterone who desire fertility, clinicians should recommend cessation of testosterone. This might allow natural endogenous production to ensue over several weeks to months. If this does not occur, clinicians can then consider human chorionic gonadotropin therapy to stimulate testicles to produce endogenous testosterone.18
Treatment of retrograde ejaculation: Retrograde ejaculation deserves special mention, given that men with this condition do not have derangement of their HPG axis or an inability to produce healthy sperm via spermatogenesis. Rather, their issue is the inability to ejaculate properly. Self-reports of low or absent ejaculation, causal medications (α-blocker medications), medical conditions (eg, diabetes mellitus), history of spinal cord injury, and relevant surgical history (bladder neck surgery such as transurethral resection of the prostate or retroperitoneal surgery) can raise suspicion in clinicians.19 Semen volumes of less than 1.5 mL should also signal this cause of male factor infertility to treating clinicians. Confirmation of retrograde ejaculation can be done through attainment of a postejaculation urinalysis, with the presence of sperm in the urine diagnostic of this condition in a man with azoospermia.19 The most commonly prescribed medications to treat this condition include as-needed pseudoephedrine or daily imipramine, while in cases of spinal cord injury either vibration- or electricity-assisted ejaculation might be required.20,21
Surgical treatment. In some patients, medical management of infertility either fails or is not possible. For these men, surgical therapies might be the only option to obtain sperm.
Varicoceles: If a man has a varicocele, abnormal semen parameters, and infertility, a varicocelectomy might be of value in improving semen parameters. Although historically this procedure was associated with some controversy given the unclear effect on pregnancy rates, a more recent meta-analysis suggests this can be an effective treatment.22
Obstructive azoospermia: For men with obstruction of the vas deferens, a vasovasostomy might be possible to bypass the obstruction. Although this procedure is commonly associated with men wishing to reverse their previously performed vasectomy, men might experience congenital or acquired causes of obstruction that can benefit from this surgery. In some instances, epididymal obstruction is present, and requires an anastomosis made directly between the epididymis and vas deferens, termed vasoepididymostomy. This procedure is much more technically demanding than the typical connection of the vas deferens and requires a skilled microsurgeon.23 Among patients whose vas deferens cannot be reconstructed or who do not wish to undergo reconstructive surgery, many techniques exist to extract sperm from the testicle or epididymis. These include noninvasive percutaneous techniques that use a needle for sperm extraction from the epididymis, testicular sperm aspiration, microsurgical epididymal sperm aspiration, and testicular sperm extraction.
Nonobstructive azoospermia: In men with nonobstructive causes of azoospermia, the most effective solution is microscopic testicular sperm extraction (mTESE). Here, with the aid of a high-powered operating microscope, an open exploration of a testicle and its seminiferous tubules can be undertaken. This allows for real-time assessment for the presence of sperm, where surgeons might spend several hours searching through the testicle to find dilated healthy seminiferous tubules that have an increased chance of containing sperm.24 With the advent of mTESE, even men with conditions traditionally associated with very poor fertility (eg, Klinefelter syndrome) now have a relatively high (44%) chance of obtaining sperm.25
If microsurgical or percutaneous techniques are used to extract sperm, couples will require further assistance through techniques such as in vitro fertilization or intracytoplasmic sperm injection (ICSI). With increasing expertise in ICSI, a fertilized embryo can now be created with as little as a single viable sperm.26 This is an important counseling point, given that assisted reproductive techniques can be expensive endeavours for patients. However, the high chance of success (there are estimates as high as 98% for attaining sperm from patients with obstructive azoospermia) for treatment of male factor infertility should be highlighted to inform our patients.1,26
Case resolution
The patient is ultimately referred to a fertility specialist who suggests that he most likely requires surgical exploration to find sperm. The couple is counseled at the time of diagnosis that despite having nonobstructive azoospermia, their chance of mTESE sperm retrieval is nearly 50%, and their chance of live birth is variable but can be approximated at 25%.27,28 They are also counseled that alternative options include sperm donation and adoption. The patient ultimately undergoes mTESE, and fortunately a small number of sperm are found; his partner undergoes egg retrieval and ICSI is carried out to achieve pregnancy.
Conclusion
This review highlights the initial evaluation of male factor infertility, which can often be performed in the primary care setting. With a careful history and judicious use of investigations, many causes of male infertility can be uncovered. Although treatment of most conditions must be done by fertility specialists, improved time to diagnosis can only benefit patients.
With currently available medical and surgical treatments, couples presenting with male factor infertility have several options to improve their chances of having a child. Although many of the treatments described above aim to improve a couple’s chances of naturally conceiving a child via intercourse, many patients ultimately require medical or surgical intervention to achieve pregnancy. This can be a long, protracted course for our patients, with important roles for primary care providers and fertility specialists alike.
Notes
Editor’s key points
▸ The diagnostic workup of men presenting with suspected infertility includes performing an in-depth history and focused physical examination. This history is largely focused on the hypothalamic-pituitary-gonadal axis and testicular development and function. Similarly, a focused physical examination can help identify potentially reversible findings (eg, varicocele).
▸ Findings of severe oligozoospermia or azoospermia should prompt a referral to a fertility specialist. Assessment of semen volume in men with azoospermia allows classification into 1 of 2 categories: low-volume or normal-volume azoospermia. Currently available medical and surgical treatments give several options to couples presenting with male factor infertility to improve their chances of pregnancy. All men should be counseled to lead a healthy lifestyle, maintain a healthy body weight, and avoid alcohol and tobacco. There are several current options for medical management of the hypothalamic-pituitary-gonadal axis, but in some cases surgical management is required to obtain sperm.
▸ Initial evaluation of male factor infertility can often be performed in the primary care setting. With a careful history and judicious use of investigations, many causes of male infertility can be uncovered. Although treatment of most conditions must be done by fertility specialists, improved time to diagnosis can help streamline care and reduce worry and stress for patients.
Points de repère du rédacteur
▸ Les examens diagnostiques pour les hommes chez qui une infertilité est suspectée comprennent une anamnèse approfondie et un examen physique ciblé. L’anamnèse se concentre principalement sur l’axe hypothalamo-hypophysogonadique, de même que sur le développement et le fonctionnement testiculaires. De même, un examen physique ciblé peut aider à cerner des conditions potentiellement réversibles (p. ex. varicocèle).
▸ Des résultats révélant une sévère oligozoospermie ou une azoospermie devraient inciter à demander une consultation spécialisée en fertilité. L’évaluation du volume de l’éjaculat des hommes souffrant d’azoospermie permet une classification en 1 de 2 catégories : l’azoospermie avec faible volume ou avec volume normal. Les traitements médicaux et chirurgicaux actuellement disponibles pour les couples en situation d’infertilité masculine offrent différentes options pour améliorer leurs chances de conception. Il faut conseiller à tous les hommes d’adopter un mode de vie sain, de maintenir un poids santé, et d’éviter l’alcool et le tabac. Il existe actuellement diverses options pour une prise en charge médicale de l’axe hypothalamo-hypophysogonadique, mais dans certains cas, une prise en charge chirurgicale est nécessaire pour obtenir du sperme.
▸ L’évaluation initiale de l’infertilité masculine peut souvent être effectuée en milieu de soins primaires. Un bilan exhaustif et un recours judicieux aux investigations peuvent permettre de découvrir de nombreuses causes de l’infertilité masculine. Même si le traitement de la plupart de ces problèmes doit être entrepris par des spécialistes en infertilité, un diagnostic plus précoce peut aider à accélérer les soins et à réduire les inquiétudes et le stress chez les patients.
Footnotes
Contributors
Both authors contributed to the conception and design of the review, administrative support, manuscript writing, and final approval of the manuscript.
Competing interests
None declared
This article has been peer reviewed.
Cet article a fait l’objet d’une révision par des pairs.
- Copyright© 2021 the College of Family Physicians of Canada
References
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.