


Abstract
Objective To describe Blueprint 2 (2018-2023), the 5-year strategic plan launched in 2018 by the Section of Researchers (SOR), as well as its guiding principles and the process used to develop it.
Composition of the committee Blueprint 2 was co-created by many stakeholders from across Canada and led by the SOR Council (SORC). The process started with an external, commissioned program evaluation in 2017 of the effect of the first SOR Blueprint (2012-2017). The findings and recommendations arising from the evaluation were presented in a day-long facilitated invitational retreat, hosted by the SORC in September 2017 and involving 40 key stakeholders.
Methods Blueprint 2 was created using a multi-pronged, participatory, and iterative process to ensure broad input and alignment with current and future opportunities and priorities.
Report Blueprint 2 incorporates 4 strategic priority areas, each supported by objectives and actions. The strategic priority areas are membership, capacity building, advocacy, and partnerships. This updated Blueprint provides a useful, membership-driven strategic plan specifically for the SOR. The implementation of its objectives will promote research and quality improvement and contribute to building a culture of curiosity. Blueprint 2 emphasizes research and quality improvement that emanate from the realities of everyday practice and are rooted in everyday work. At its core are patient- and community-oriented approaches; it also contributes to achieving the Quadruple Aim. These outcomes will further the integration of the scholar role into daily practice for family physicians and primary care clinicians and teams.
Conclusion The ability of family physicians to identify, study, and cite their own evidence is essential to establishing the value and effect of primary care, including family medicine, in relation to Canadians’ health and the Canadian health care system.
Primary care, including family medicine, is the foundation of a health care system. Improved population health outcomes are most closely associated with countries that have the strongest primary care systems; strong primary care health services improve the overall health and longevity of the population, reduce inequity in the distribution of health care, and help to reduce costs.1,2 Various components of primary care—health promotion, illness and injury prevention, and diagnosis and treatment of illness—contribute to these desirable outcomes, as do primary care’s key characteristics of generalism, continuity, comprehensiveness, coordination of care, and first-contact and patient-centred care. Primary care, in turn, falls within the wider concept of primary health care, which, as defined by the World Health Organization, is
essential health care based on practical, scientifically sound and socially acceptable methods and technology made universally accessible to individuals and families in the community through their full participation and at a cost that the community and country can afford to maintain at every stage of their development in the spirit of self-reliance and self-determination.3
In Canada and internationally, much of the body of work that has contributed to understanding the role of primary care and primary health care has been generated by research teams that have included family medicine or primary care researchers. In addition to their work researching health services and systems, primary care researchers have also been undertaking research within other domains, such as clinical care, education, population health, and Indigenous health. Asking and systematically answering research questions in these domains creates the evidence for the specialty that is family medicine, influences education and care, and transforms health services. Research is, therefore, recognized as a key role in the College of Family Physicians of Canada (CFPC) Family Medicine Professional Profile.4
With the goal of advancing primary care research, the CFPC established a Section of Researchers (SOR) in 1995, which now constitutes a large community of more than 1600 family medicine and primary care researchers across Canada. In 2018, the SOR launched its new strategic plan, Blueprint 2, for the 5-year period from 2018 to 2023, replacing its original SOR Blueprint (2012 to 2017). This revised plan, its guiding principles, and the process used to develop it are described in this article.5
Composition of the committee
Following an external, commissioned program evaluation in 2017 of the effect of the first SOR Blueprint, Blueprint 2 was co-created by multiple stakeholders from across Canada using a multi-pronged, participatory, and iterative process to ensure broad input and alignment with current and future opportunities and priorities. It was led by the SOR Council (SORC) and is aligned with the CFPC’s mission of improving lives and its overall strategic plan.6
Methods
The development process started with an external, commissioned program evaluation in 2017 on the effect of the first SOR Blueprint. The process included interviews with key informants and an assessment of deliverables, products, and other indicators, using a logic model that had been developed at the outset of the first Blueprint. The findings and recommendations that emanated from the evaluation were presented in a day-long facilitated invitational retreat, hosted by the SORC in September 2017 and involving 40 key stakeholders. Participants represented various levels of expertise, professions, and perspectives related to primary care research; 80% were family physicians and 20% were non–family physicians. This meeting and follow-up deliberations by the SORC contributed to identifying general principles, directions, and priorities for Blueprint 2. An ad hoc working group was struck to collate the input received and to draft Blueprint 2. An iterative process followed that involved face-to-face meetings, videoconferences, and further input from more than 70 key informants. The informants were identified by purposive sampling and included, among others, family medicine residents, family medicine clinicians engaged in research, primary care researchers, and research leaders.
Report
Guiding principles. Several guiding principles informed the creation of Blueprint 2. Foremost was the recognition that primary care research is not undertaken only by full-time researchers; it can and should include participation by many others, including clinicians at the front lines of care. Clinician scientists and researchers, with their advanced training and experience in research, lead research endeavours. Further, more research training and resources are required to ensure primary care research continues to grow and develop. Advocacy for these much-needed research training opportunities and resources is a core activity in Blueprint 2.
Research represents a broad spectrum of activities that offer opportunities for all, including many who might not describe themselves as researchers.7 These activities include searching for evidence to inform responses to questions from everyday practice; critically appraising evidence; developing clinical guidelines, knowledge syntheses, case reports, and case studies; contributing data to practice-based research and quality improvement (QI) networks; recruiting patients to studies; and participating in or leading research using a variety of methods (quantitative, qualitative, and mixed-methods) and designs (from retrospective studies to randomized controlled trials).
Blueprint 2 recognizes the contributions and importance of every one of these activities because each, in its own way, contributes to the evidence used in the disciplines of family medicine and primary care and to patient care and practice improvement. Blueprint 2 particularly emphasizes the opportunity for many more clinicians to make additional use of their practice data for the purposes of practice improvement and to connect with research networks, such as practice-based research networks (PBRNs) and the Canadian Primary Care Sentinel Surveillance Network. These networks can provide useful feedback to individual clinicians and practices that results in practice improvement, while also adding research capacity.
Blueprint 2 recognizes the important contributions of research, local data, and QI initiatives to practice improvement. Although they are different approaches, they have substantial overlap and all contribute to a culture of curiosity in family medicine and primary care. This strong synergy leads, in turn, to improvements in practice and education, often arising from within family practice clinics and teams. This aspect of Blueprint 2 is inspired by Mold and Peterson’s vision of learning networks8 in which clinicians, patients, researchers, and QI champions collaborate, using their different approaches to effect practice improvement and fulfil the Quadruple Aim9 (namely, to continually improve care, the patient experience, efficiencies, and the work experience of health care providers). To advance this concept, the CFPC and the SORC are advocating for the co-creation of the next iteration of PBRNs—namely, practice-based learning networks (PBLNs).
Four strategic priority areas. Blueprint 2 incorporates 4 strategic priority areas—membership, capacity building, advocacy, and partnerships—each supported by objectives (Figure 1) and actions.5
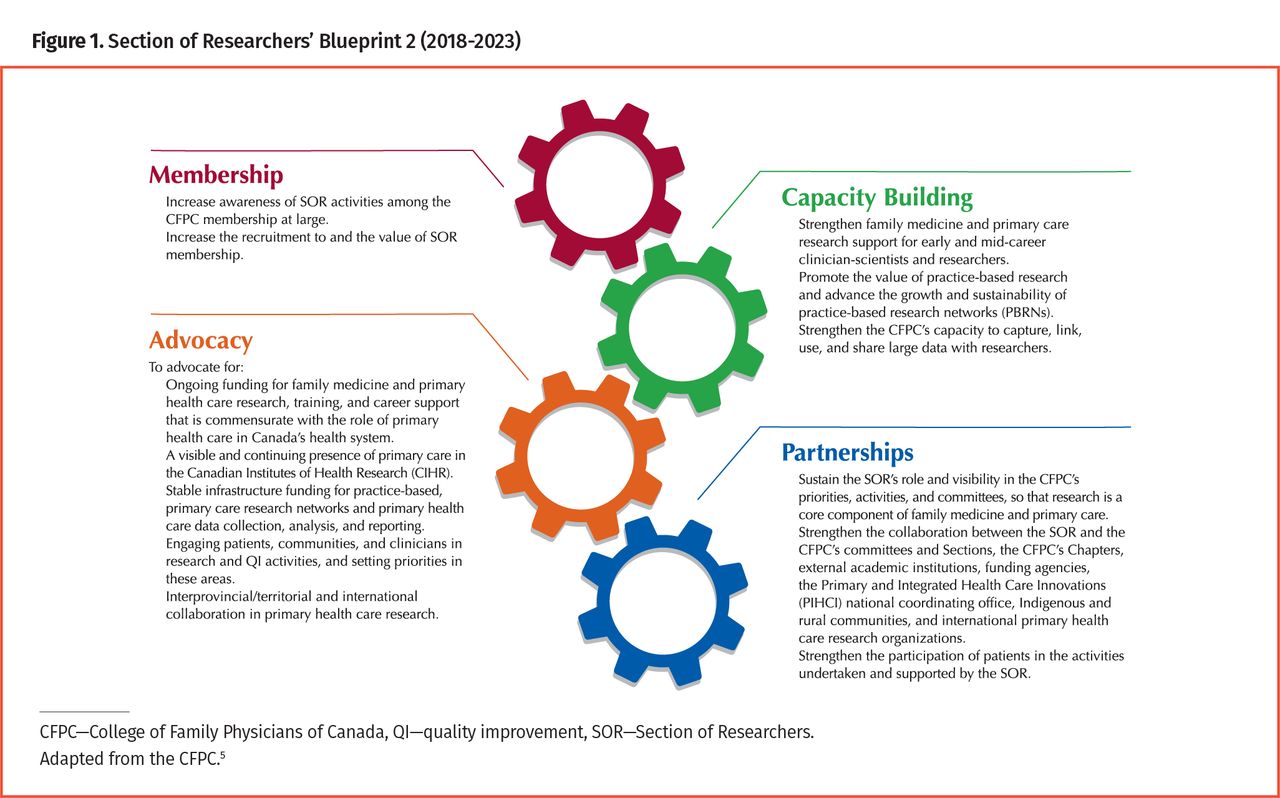
Section of Researchers’ Blueprint 2 (2018-2023)
Membership. Growing the membership base and increasing awareness of primary care research and the SOR among family physicians, residents, and primary care colleagues remain strategic priorities. A specific focus is to highlight the added value of membership in the SOR by increasing the presence of the SOR on social media, on the CFPC website, and in Canadian Family Physician; enhancing communication with members; inviting membership from groups and organizations involved in primary health care research; reviewing and enhancing the benefits for all categories of membership; and increasing the number of research- and QI-related awards.
Capacity building. Research and practice improvement are not possible if the necessary capacity for engagement in these activities is lacking. The previous Blueprint saw successes in a number of areas in this domain, including increasing research content in family medicine residency training curricula, making research more explicit in the accreditation of residency programs, and making research a cornerstone activity in the CFPC’s annual Family Medicine Forum. Blueprint 2 will build on these successes and encourage engagement in research activities earlier in members’ careers, promote research and the use of data for research and QI at a practice level, and advance the use of big data in undertaking research.
Blueprint 2 outlines several activities to achieve these objectives: promoting the use of data that support research and QI at a practice level, and providing Mainpro+® credits for such activities; supporting and promoting research training and capacity-building programs; establishing a research community of practice and a virtual knowledge and innovations hub that connects SOR members; promoting family medicine and primary health care research among medical students and family medicine residents; promoting and strengthening primary care PBRNs and PBLNs across Canada; and supporting the development of a primary care research institute to facilitate the CFPC’s ability to make big data available to researchers.
Advocacy. Despite primary care being a cornerstone of the health care system, research in this area has been underfunded and underresourced in Canada. Advocacy remains paramount to raising awareness, visibility, and support. Blueprint 2 urges advocating for increased funding and infrastructure for family medicine and primary care research and QI. The SOR will also continue to advocate for ensuring access to electronic medical record data in support of research and QI at the practice level.10
Specific actions will include developing a proposal for a Canadian Institutes of Health Research (CIHR) institute of integrated primary home and community health care research; advocating that the CIHR and other research funders support systematic tracking and annual reporting of all primary health care research funding; advocating for sustainable infrastructure support for PBRNs and PBLNs, as well as for primary health care data collection, analysis, and reporting; promoting and supporting patient and community engagement in research and QI; advocating that the CIHR and other research funders, as well as researchers and research organizations, support primary health care research collaboration among the provinces and territories and internationally; and supporting provincial Chapters, department chairs, research directors, and SORC members in advocacy efforts at the provincial or territorial level and, where appropriate, at the federal level.
Partnerships. Primary care research is a collaborative effort. Collaboration occurs within and across teams, and across organizations and jurisdictions. Strengthening existing partnerships and establishing new links supports many of the other Blueprint 2 objectives. Successful partnerships from the initial Blueprint can be strengthened and leveraged in many ways: by partners being involved on various committees and task forces, so as to integrate various aspects of research and QI efforts into training, education, scholarship, and practice; by further developing research partnerships with other primary health care professional organizations; by further developing partnerships with provincial and national organizations and agencies that use big data; by inviting Indigenous family physicians and researchers, and individuals from Indigenous communities, to participate in the activities of the SOR, including the SORC; and by working with the CIHR, other research funders, researchers, research organizations, CFPC Chapters, and international partners to promote and support interprovincial and international primary health care research collaborations.
Next steps. Dissemination of Blueprint 2 is under way using various strategies, including presentations to the 17 departments of family medicine at universities across Canada, to various CFPC partner and sister organizations, and at several primary care conferences. French and English versions are available on the CFPC website (https://www.cfpc.ca/en/member-services/committees/section-of-researchers-council). An evaluation framework, including outcome measures and indicators of success for each strategic priority area, will complement Blueprint 2 and help the SORC monitor the progress and effect of its strategic plan.
Conclusion
Blueprint 2 (2018 to 2023) has something for everyone and provides a useful, membership-driven strategic plan for the SOR. The implementation of the objectives will promote research and QI and contribute to building a culture of curiosity. Blueprint 2 emphasizes research and QI that arise from everyday practice and are rooted in everyday work, including the questions that family physicians and their primary care colleagues encounter at the front lines of care. At the core of Blueprint 2 are patient- and community-oriented approaches, which contribute to achieving the Quadruple Aim.9 These outcomes will also contribute to the integration of the scholar role into the daily practice of family physicians and primary care clinicians and teams.
Establishing the effect of primary care, including family medicine, on Canadians’ health and the value it brings to the Canadian health care system depends on our ability to identify, study, and cite our own evidence. The SOR’s Blueprint 2 (2018 to 2023) recognizes this reality and articulates a plan to help us achieve this vision.
Acknowledgment
The authors acknowledge Tinu Ojikutu, Research Coordinator of the Section of Researchers, for her collaboration throughout the entire process of co-developing and disseminating Blueprint 2, and the many stakeholders who generously gave their time and helpfully responded to our request for reviews and comments.
Notes
Editor’s key points
▸ Family physicians in Canada need to be able to identify, study, and cite research that emanates from the realities of their everyday practice.
▸ Primary care research can and should include participation by clinicians at the front lines of care.
▸ Blueprint 2 (2018 to 2023) has something for everyone and provides a useful, membership-driven strategic plan for the Section of Researchers of the College of Family Physicians of Canada. The implementation of the objectives will promote research and quality improvement and contribute to building a culture of curiosity. These outcomes will also contribute to the integration of the scholar role into the daily practice of family physicians and primary care clinicians and teams.
Points de repère du rédacteur
▸ Les médecins de famille au Canada doivent pouvoir définir, étudier et citer la recherche qui émane des réalités de leur pratique au quotidien.
▸ La recherche en soins primaires peut et devrait inclure la participation des cliniciens sur la première ligne des soins.
▸ Le Plan directeur 2 (2018 à 2023) a quelque chose pour tous et présente un plan stratégique utile, dirigé par des membres, pour la Section des chercheurs du Collège des médecins de famille du Canada. La réalisation des objectifs favorisera la recherche et l’amélioration de la qualité, et contribuera à créer une culture de curiosité. Ces accomplissements aideront aussi à intégrer le rôle d’érudit dans la pratique au quotidien des médecins de famille ainsi que des équipes et des cliniciens de soins de première ligne.
Footnotes
Contributors
All authors contributed to the literature review and interpretation, and to preparing the manuscript for submission.
Competing interests
None declared
- Copyright© the College of Family Physicians of Canada





{kind=link}