


Abstract
Objective To understand physician acceptance of new patients, specifically the use of “meet and greets”; and to explore FPs’ rationale, beliefs, and processes regarding these appointments.
Design Exploratory qualitative interviews.
Setting Nova Scotia.
Participants A purposive sample of 12 FPs who had previously participated in the Models and Access to Primary Care Providers in Nova Scotia study.
Methods In-depth, semistructured, 1-on-1 qualitative interviews. Interview transcripts were coded using Atlas.ti and analyzed for typologies and common themes regarding accepting practices.
Main findings Four typologies of accepting practices emerged: no form of meet and greet; nonscreening meet and greet to gather a history; meet and greet to assess alignment of patient needs and provider scope; and meet and greet to screen out undesirable patients. Typology 1 was subdivided: accepting first-come, first-served and accepting with previous patient knowledge. Rationale for each varied. Family physicians employing typologies 1 and 2 emphasized the importance of equitable access to primary care. Family physicians employing typologies 3 and 4 highlighted the challenges of meeting the needs of specific populations within the context of professional and systemic constraints.
Conclusion Meet and greets before accepting new patients are purposed differently across providers. Some FPs incorporate these meetings ethically; others present challenges to the principles of equity and nondiscrimination. Policy implications exist for how providers admit new patients and what resources might support more equitable access.
Primary care is the main point of entry into the Canadian health care system. The Canadian Medical Association mandates that physicians accept new patients in a fair and equitable manner.1 Many provincial colleges of physicians and surgeons support this through policy statements recommending physicians accept patients on a “first-come, first-served” basis.2-4 Despite these policies, individuals seeking FPs have reported practices where providers meet with them to collect a thorough history, then appear to accept or decline them based on the “meeting.”5 These initial meetings are often referred to as “meet and greets.”
Meet and greets can be used for information exchange, to facilitate the formation of a patient-provider relationship, and to ensure the patient’s needs fall within the provider’s scope of practice. However, meet and greets can potentially be abused as unethical screening tools to identify preferable patients. These practices have been colloquially referred to as “cherry picking”— accepting “easy” patients into practice—or “lemon dropping”—denying more “challenging” patients.6
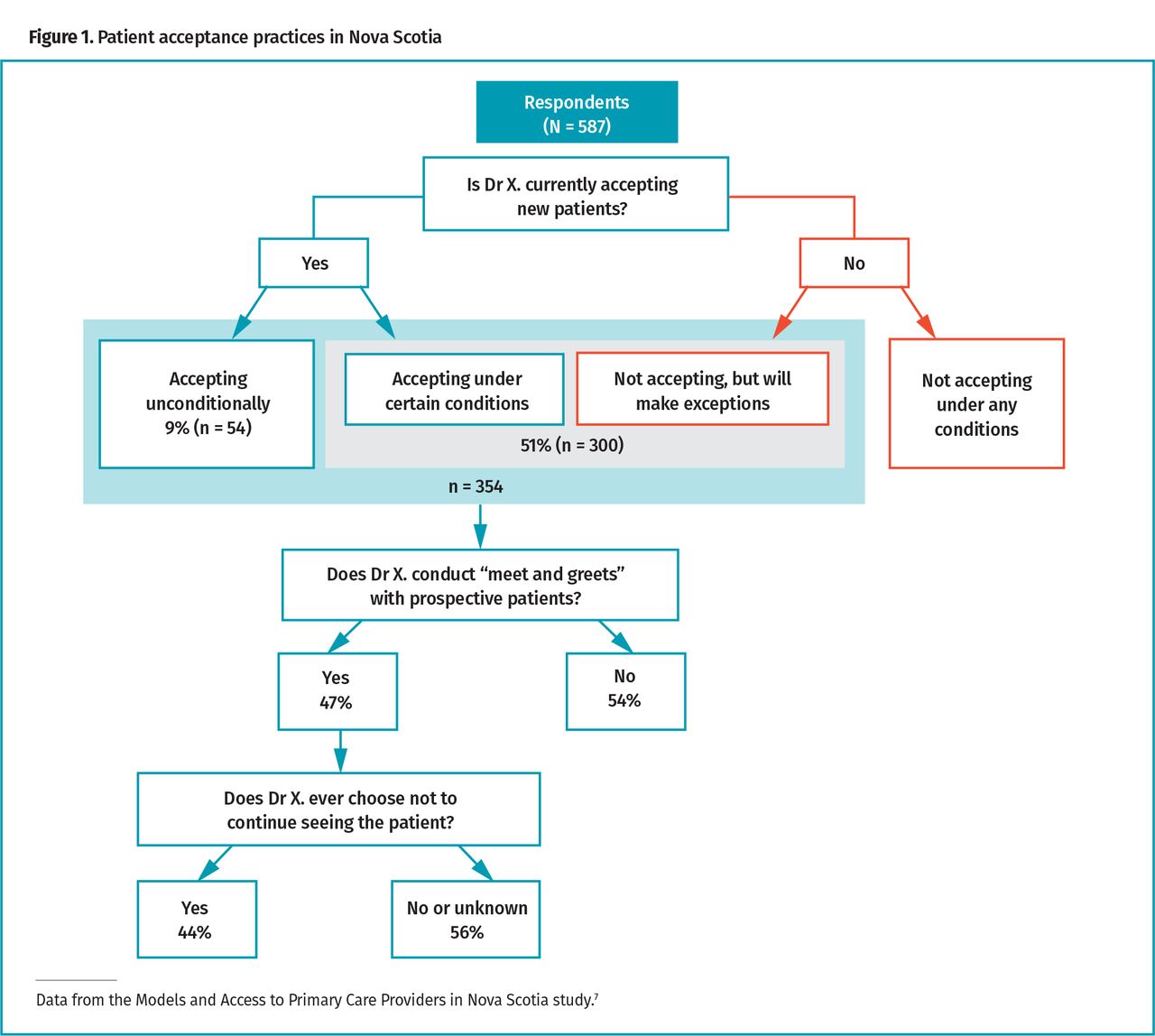
Previously published findings from the Models and Access to Primary Care Providers in Nova Scotia (MAAP-NS) study describe the prevalence of meet and greets in Nova Scotia.7 Eighty-four percent (n = 587) of FPs in the province participated in the study. Of those, less than 10% were accepting new patients unconditionally. Several physicians stated that they accepted new patients, but only under certain conditions—such as pregnancy—while those who were not accepting new patients noted that they made exceptions. Thus, 354 FPs (about 51%) will accept new patients either unconditionally or with conditions or exceptions. Interestingly, of this cohort, nearly half (47%, n = 166) said they required a meet and greet before initiating a therapeutic relationship. Furthermore, as many as half of the providers conducting meet and greets reported at least once discontinuing seeing a potential new patient following this interview.7 Figure 1 illustrates these acceptance practices.7
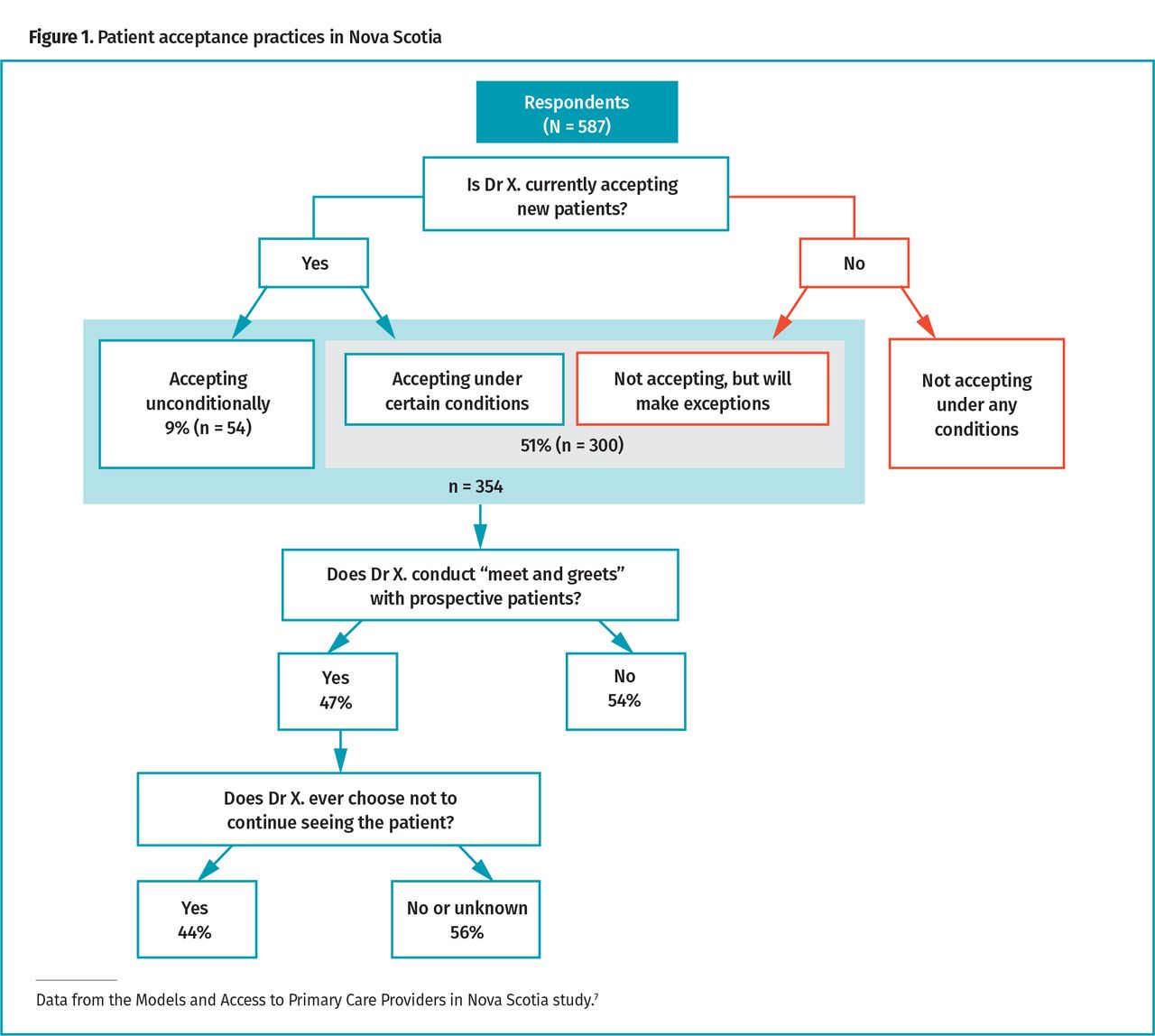
Patient acceptance practices in Nova Scotia
While screening patients can be viewed as unethical, it is also in direct contravention of the policy statements of several provincial colleges of physicians and surgeons and the Canada Health Act.2,4,8-10 In 2017, Statistics Canada estimated that 13.1% of Nova Scotia residents older than 12 years of age did not have access to a regular FP.11 The low numbers of FPs accepting patients, coupled with the concurrent proportion of unattached patients, adds to the importance of understanding the decision-making practices related to patient attachment to a regular FP.
Given how little is known about meet and greets and the potential for them to be used for, or perceived as, a screening mechanism, further exploratory investigation is warranted. This study seeks to enhance understanding of the purpose, goals, and outcomes of meet and greets from the perspective of FPs.
Methods
An exploratory qualitative description study design12 was employed to guide our focused inquiry of meet and greets in family practice. Qualitative description is the method of choice when straight descriptions of a phenomenon are desired—in this case, the phenomenon of meet and greets.12 One author, V.S., who was a master’s-prepared medical student at the time, conducted in-depth, 1-on-1 interviews with 12 FPs. Her qualitative interview experience also came from previous work as an interviewer in a national mixed-methods study funded by the Government of Canada,13 and was further supplemented by discussion with the experienced supervising co-author (E.G.M.). A semistructured interview guide was used to uncover the nuances of meet and greets (available on request). Only FPs who had previously participated in the MAAP-NS study and had consented to being contacted for follow-up research were approached. Use of data from the MAAP-NS study facilitated a purposive sampling strategy to target potential key informants and maximize variability, as is appropriate for qualitative description design,12 with respect to provider sex, years in practice, and use of meet and greets in practice. Saturation, a process by which the investigators agreed that no new narratives were emerging, was achieved after 10 interviews; 2 additional interviews, for a total of 12, confirmed saturation.
Interviews were audiorecorded and transcribed verbatim. The authors used qualitative data analysis software (Atlas.ti) to independently code transcripts for emerging themes. Through successive meetings, consensus was reached on the typologies and common themes.
Ethics approval was received from the Nova Scotia Health Authority.
Findings
Study participants were all practising FPs in Nova Scotia at the time of the interviews. Two-thirds (n = 8) of participants were women. Years in practice ranged from 3 to more than 35. One-third (n = 4) of participants were remunerated via alternative funding plans and the remaining were paid by fee-for-service. One participant was from a rural area. Seven participants reported using meet and greets during the MAAP-NS survey, although qualitative inquiry revealed nuance to this. Demographic characteristics of participants can be found in Table 1.7
Participant characteristics: N = 12.
Conversations with FPs revealed that while the phrase meet and greet is familiar, there is no common definition and the term applies to a variety of practices with potential new patients. While some providers use meet and greets in practice, the purpose differs. Each of our participants fell into 1 of 4 mutually exclusive typologies with respect to meet and greets, which are discussed in detail below. Table 2 provides quotations illustrating the typologies.
Examples from each typology
Typologies
Typology 1—no meet and greet
These FPs do not use meet and greets when accepting new patients. They report deciding at the time of request whether they can accept new patients based on their current personal and professional burden. Some cited ethical considerations such as “cherry picking” and discrimination as reasons for not using meet and greets. Some interviewees discussed the ineffectiveness of meet and greets as a screening tool, while others did not want to be perceived as screening patients. Two subtypes exist within typology 1.
Subtype 1A—accepting first-come, first-served: When a provider’s practice is open, they accept patients on a first-come, first-served basis, with no prior knowledge of the patients. No participants had an open practice, but nearly all interviewees using typologies 1 and 2 used this approach to initially build their practices. Interviewees noted they would make exceptions to their “closed practice” for family members of current patients—a practice supported by the College of Physicians and Surgeons of Nova Scotia (CPSNS).2
Subtype 1B—accepting with prior patient knowledge: Sometimes, despite having a “closed” practice, interviewees still accept new patients on an ad hoc basis depending on the medical concern or referral source. Examples include patients in need of prenatal care, patients whose FP recently retired or passed away, Francophone patients (when the provider is also Francophone), or patients referred from colleagues.
Typology 2—meet and greet to gather medical history
Typology 2 FPs use meet and greets at the outset of the patient-provider relationship, but only after accepting the patient into practice. These meetings are used to collect a history, initiate a rapport between patient and provider, and familiarize the patient with the care team and practice policies. Some providers noted that if there was an active medical issue at hand, the meet and greet would occur during the patient’s first appointment. Typology 2 providers highlight similar themes regarding equity and lack of discrimination in accepting patients as those in typology 1. They emphasize that the purpose of meet and greets is entirely informative and does not affect the patient’s acceptance. However, several highlighted that this initial meeting allows patients to decide if they are comfortable with the practice model and care goals, and whether they want to continue a patient-provider relationship.
Typology 3—meet and greet to assess alignment of patient needs and provider scope
These FPs describe meeting with prospective patients to discuss the scope and limitations of their practice before accepting them as patients. They assess patient needs to evaluate suitability of the potential patient-provider relationship. Some providers use this time to tell patients they do not offer certain services.
Typology 4—meet and greet to screen out undesirable patients
These FPs use meet and greets to screen out “undesirable patients.” Providers meet with patients to learn their medical needs and decide whether to accept them into practice. Undesirable patients were those perceived to be “doctor shopping,” opioid seeking, having difficult personalities, or requiring complex care. Some providers highlighted their desire for professional autonomy as a reason for interviewing patients. Colleagues employing typologies 1 and 2 corroborated the challenges associated with these patients, although they emphasized that patients with complex issues are often the most in need of care and, as such, screening them out of practices is discriminatory and detrimental to their health.
Cross-cutting themes
Three cross-cutting themes exist among practitioners regardless of the typology they subscribe to: ethics of practice, compromises of practice, and freedom of practice. These themes are illustrated in Table 3.
Cross-cutting themes
Ethics of practice was discussed among interviewees using typologies 1, 2, and 3. Providers describe not only the impact on the patient who might be screened out, but also professional standards and access issues that might arise within the health care system secondary to employing screening meet and greets. Providers using typology 4 did not mention ethical principles in relation to meet and greets.
All interviewees discussed compromises of practice associated with the burdens of accepting certain patient types and remuneration models. These burdens incentivize some providers to restrict entry to their practices. Other providers compromise financial gain to ensure access for patients. Antiquated billing codes and fee-for-service remuneration were identified as motives for screening patients, as they do not appropriately compensate for the time and effort often demanded by complex patients. Providers note maintaining accessibility for current patients, striving for work-life balance, and having capacity to financially sustain their practices as challenges in serving an increasing number of complex patients. Some suggest that providing equitable, high-quality care and earning appropriate compensation are mutually exclusive.
Participants discussed empowerment, or freedom of practice, in their practice decisions, including how they accept new patients, and their practice scope and limitations. This privilege of choice is considered a unique aspect of family practice and a selling feature of the profession used to recruit new physicians. This might result in a disservice to equity and access in care, as providers feel entitled to this privilege.
Discussion
Typology 1 FPs highlight ethical issues associated with selecting patients and a desire to serve all patient populations regardless of the associated challenges. Some providers consider meet and greets futile owing to the inability to predict who will become “undesirable.” We posit that typology 1A represents the acceptance practice with the fewest ethical problems,7 as practices are either open or closed irrespective of patient history. We speculate that typology 1B has the potential to be used as an indirect screening method, as patient information could inform acceptance decisions. Providers themselves identified this ethical hiccup when analyzing their acceptance practices.
Typology 2 FPs use meet and greets solely for welcoming patients, familiarizing them with the practice, and collecting a history. It is possible that meet and greets may facilitate a strong patient-provider relationship and better prepare physicians for the needs of their new patients. However, regardless of intent, patients might be intimidated by this initial appointment.10 Thus, it is important providers clarify that patients have already been accepted when inviting them for this appointment.
Typology 3 represents an ethical challenge and conflicts with the policies and guidelines of several colleges of physicians and surgeons. These stipulate that scope of practice limitations are permissible grounds for restricting patient entry to practice; however, these limitations should be communicated to patients before conducting any meetings with them.1,3,4,9 Thus, meet and greets to assess the “fit” between providers and patients should not be occurring in Nova Scotia, and providers with scope of practice limitations should delineate these to all prospective patients before arranging an introductory appointment, as per CPSNS guidelines.2 Greater transparency around their practice scope and timely provision of this information to prospective patients could prevent these physicians from being perceived as discriminatory, regardless of intent. Furthermore, the CPSNS states that when a physician’s scope of practice limits their ability to meet patient needs, it is their duty to refer to another provider. Only 1 interviewee cited doing so.
It is appropriate to conclude that typology 4 FPs are acting in direct contravention of the minimum ethical and professional behaviour expected of physicians, given the explicit standards outlined by the CPSNS and the Canada Health Act. Typology 4 FPs suggest time constraints, increasingly complex patients, and preserving their own well-being as the motivators for cherry picking patients.
Most providers describe the influence of ethical considerations on accepting practices, and all identify challenges that could pressure a provider to modify these practices. We posit that most meet and greets evolved not to screen out challenging patients simply for ease of practice, but as a means for physicians to continue providing high-quality care within the context of systemic limitations and financial burdens. While there is no acceptable reason for discriminating against patients, developing an understanding of the root causes of this behaviour can inform systemic changes that can better support a climate of equity. Freedom of practice permeated discussion in a way that we posit is unique to family medicine. Non-FP specialists, for example, are not able to screen out complex or challenging patients and cannot close their practices secondary to personal or professional strains. It is worth considering this freedom of choice within a practice model—often presented as a selling feature of the profession—might contribute to a climate of inequity.
The CPSNS suggests that should “introductory meetings” be held after accepting patients into practice (ie, typology 2), it is recommended that physicians advise patients of the purpose of the appointment, not bill for this time, and follow relevant legislation around privacy and documentation.2 It is unclear whether typology 2 physicians bill for this meeting if medical issues are not addressed. Given that interviews within typologies 3 and 4 should not be occurring, they certainly should not be billed for.
Limitations
The number of participants (N = 12) may be cited as a limitation; however, this is typical for in-depth qualitative inquiry focused on a narrow topic from a small population (Nova Scotia has approximately 1300 FPs, some of whom work in focused practice14). The assurance of representation is strengthened by the recruitment strategy facilitated by the principal investigator of the MAAP-NS study, whereby participating FPs had signed a consent form to be contacted for future research. Data from MAAP-NS were used to purposively sample a diverse range of FPs.
Conclusion
To our knowledge, this is the first study to explore FPs’ processes and reasons for conducting meet and greets before accepting patients into their practices. We provide novel information that not all meet and greets are equivalent and that defining them solely by their colloquial term may misconstrue parameters of concern.
While meet and greets are a common practice in Nova Scotia, and likely other jurisdictions, this initial investigation suggests that the motivation behind them is complex. Economic burden and professional burnout factor into the decision to tailor one’s practice. However, meet and greets might have a disproportionately negative effect on patients who require the most care, potentially further disadvantaging vulnerable populations. Additionally, cherry picking patients shunts the burden of complex and time-consuming care to physicians who are not participating in screening processes. These findings are worrisome when considered in the context of high volumes of unattached patients and few “open” family practices. A clear understanding of the factors influencing the use of these meetings can guide policy interventions to maximize accessibility and provider support. Consultation with front-line physicians regarding practical changes that could be implemented to stymie these unethical practices warrants further investigation in order to benefit both patient access and provider wellness.
Acknowledgment
This study was funded by the Nova Scotia Health Research Foundation and the Dalhousie University Faculty of Medicine Creighton Family Rural Summer Studentship. We thank the family physicians who participated in this research.
Notes
Editor’s key points
▸ The Canadian Medical Association mandates that physicians accept new patients in a fair and equitable manner, yet some individuals seeking FPs have reported practices where providers meet with them to collect a thorough history, then appear to accept or decline them based on this “meet and greet.”
▸ Previous research indicated that about half of FPs in Nova Scotia will accept new patients either unconditionally or with conditions or exceptions, and of those physicians, nearly half require meet and greets. This qualitative study aimed to enhance understanding of the purpose, goals, and outcomes of meet and greets from the perspective of FPs in Nova Scotia.
▸ While meet and greets are a common practice in Nova Scotia, and likely other jurisdictions, this initial investigation suggests that the motivation behind them is complex. Economic burden and professional burnout factor into the decision to tailor one’s practice. However, meet and greets might have a disproportionately negative effect on patients who require the most care, potentially further disadvantaging vulnerable populations. Additionally, cherry picking patients shunts the burden of complex and time-consuming care to physicians who are not participating in screening processes.
Points de repère du rédacteur
▸ L’Association médicale canadienne impose que les médecins acceptent de nouveaux patients de manière juste et équitable, et pourtant, certaines personnes en quête d’un MF ont signalé des pratiques selon lesquelles les médecins les rencontraient pour effectuer une anamnèse en profondeur, puis semblaient les accepter ou les refuser en se basant sur ces rencontres d’accueil.
▸ Des recherches antérieures ont indiqué qu’environ la moitié des MF en Nouvelle-Écosse accepteront de nouveaux patients, soit inconditionnellement, ou en fonction de certaines conditions ou exceptions, et parmi ces médecins, près de la moitié exigent une rencontre d’accueil. Cette étude qualitative avait pour but de mieux comprendre la raison d’être, les objectifs et les résultats de ces rencontres du point de vue de médecins de famille en Nouvelle-Écosse.
▸ Même si les rencontres d’accueil sont une pratique courante en Nouvelle-Écosse et probablement dans d’autres régions, cette investigation initiale porte à croire que la motivation sous-jacente est complexe. Le fardeau économique et l’épuisement professionnel sont pris en compte dans la décision de définir sa propre pratique. Par ailleurs, les rencontres d’accueil pourraient avoir des effets négatifs disproportionnés sur les patients qui ont le plus besoin de soins, et peut-être désavantager encore plus les populations vulnérables. En outre, l’acceptation sélective des patients fait porter le fardeau des cas complexes et qui demandent beaucoup de temps sur les épaules de médecins qui ne procèdent pas à des processus de sélection.
Footnotes
Contributors
Dr Emily Gard Marshall conceptualized and designed the study. Dr Victoria Smith recruited participants, conducted the interviews, transcribed most of the interviews, and co-wrote the manuscript with Dr Emily Gard Marshall. Both authors reviewed and analyzed the transcripts and approved the final version of the manuscript for submission.
Competing interests
None declared
This article has been peer reviewed.
Cet article a fait l’objet d’une révision par des pairs.
- Copyright © the College of Family Physicians of Canada
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.