


Abstract
Objective To provide recommendations for management of patients presenting with elevated self-administered bleeding assessment tool (Self-BAT) scores or other bleeding symptoms in a primary care setting.
Sources of information Primary research sources, clinical review articles, and interviews with research staff, hematologists, and family physicians were used to create the poster tools and reference guide resources.
Main message Recommendations to manage a patient with an elevated Self-BAT score or other bleeding symptoms include reviewing the results of the Self-BAT to clarify relevant symptoms, performing initial diagnostic laboratory tests, and doing basic symptom management. Clinical judgment should be used when determining whether referral to a hematologist is necessary, but referral should be considered if the bleeding score is abnormal or if initial management options are ineffective. Some bleeding symptoms warrant evaluation by a gastroenterologist, obstetrician-gynecologist, or otolaryngologist.
Conclusion Primary care providers should conduct a thorough review of the Self-BAT results and associated management recommendations when working with a patient presenting with an elevated score or other bleeding manifestations. A review consists of the clarification of relevant symptoms, appropriate initial laboratory workups, and patient education. Treatment options for symptom management should be explored while recognizing the threshold for referral to a hematologist.
Symptomatic inherited bleeding disorders are common in the Canadian population, with a prevalence of approximately 1 in 1000.1 Bleeding disorders such as von Willebrand disease (VWD) are characterized by excessive and-or prolonged bleeding caused by minor wounds, dental work, or procedures and surgery; easy bruising; epistaxis; oral cavity bleeding; and musculoskeletal bleeding in severely affected individuals.1,2 Additionally, women in particular may experience menorrhagia, postpartum hemorrhage, and other obstetric and gynecologic symptoms.3,4
Despite the negative impact of bleeding symptoms, there remain multiple obstacles to diagnosis owing to difficulties in reporting hemorrhagic symptoms and in differentiating between normal and abnormal bleeding.5,6 Women are disproportionately affected as gynecologic and obstetric manifestations of bleeding disorders are often difficult to quantify and are frequently overlooked or dismissed.1 Without recognition of abnormal symptoms, many affected women are left undiagnosed and without appropriate management.7,8 This results in decreased health-related quality of life.9,10
Furthermore, lack of international consensus surrounding diagnostic thresholds, classification, and nomenclature poses further barriers to effective bleeding assessment and subsequent management. Recent efforts to improve risk assessments and diagnostic accuracy and to inform referrals and treatments have led to the development and recognition of standardized bleeding assessment tools (BATs) for use in screening and diagnosis.1 Validated BATs are helpful tools for supplementing patient history and informing referral.11,12 Developed by the International Society on Thrombosis and Haemostasis (ISTH) in 2010, the ISTH-BAT provides a series of questions and scores to standardize quantitative reporting of bleeding symptoms.13-15 However, as the ISTH-BAT was designed to be a screening tool administered by health care professionals, it was initially inaccessible for widespread public use.
In 2015 the self-administered BAT (Self-BAT) was introduced, providing modifications to the ISTH-BAT and enabling the general public to determine their bleeding scores independently in layperson terms. While there are limitations to the Self-BAT format, such as its reliance on recall and risk of score saturation leading to under-reporting of bleeding symptoms, the Self-BAT has been validated as a screening tool for underlying bleeding disorders.16 Bleeding assessment tools accurately distinguish between normal and abnormal bleeding and are recommended for use in primary care settings by the American Society of Hematology, ISTH, National Hemophilia Foundation, and World Federation of Hemophilia 2021 guidelines.17
The promotion of the Self-BAT through the Let’s Talk Period website (https://letstalkperiod.ca) in 2016 enabled widespread availability of the tool to the general public. In addition to increasing public accessibility and awareness of the Self-BAT, the website simultaneously functions as a knowledge translation tool by presenting information on normal versus abnormal menstrual bleeding.18 Let’s Talk Period has been promoted in the news, social media, and classrooms. A total of 19,365 individuals had completed the Self-BAT as of 2020, with 44% having obtained an abnormal bleeding score.1
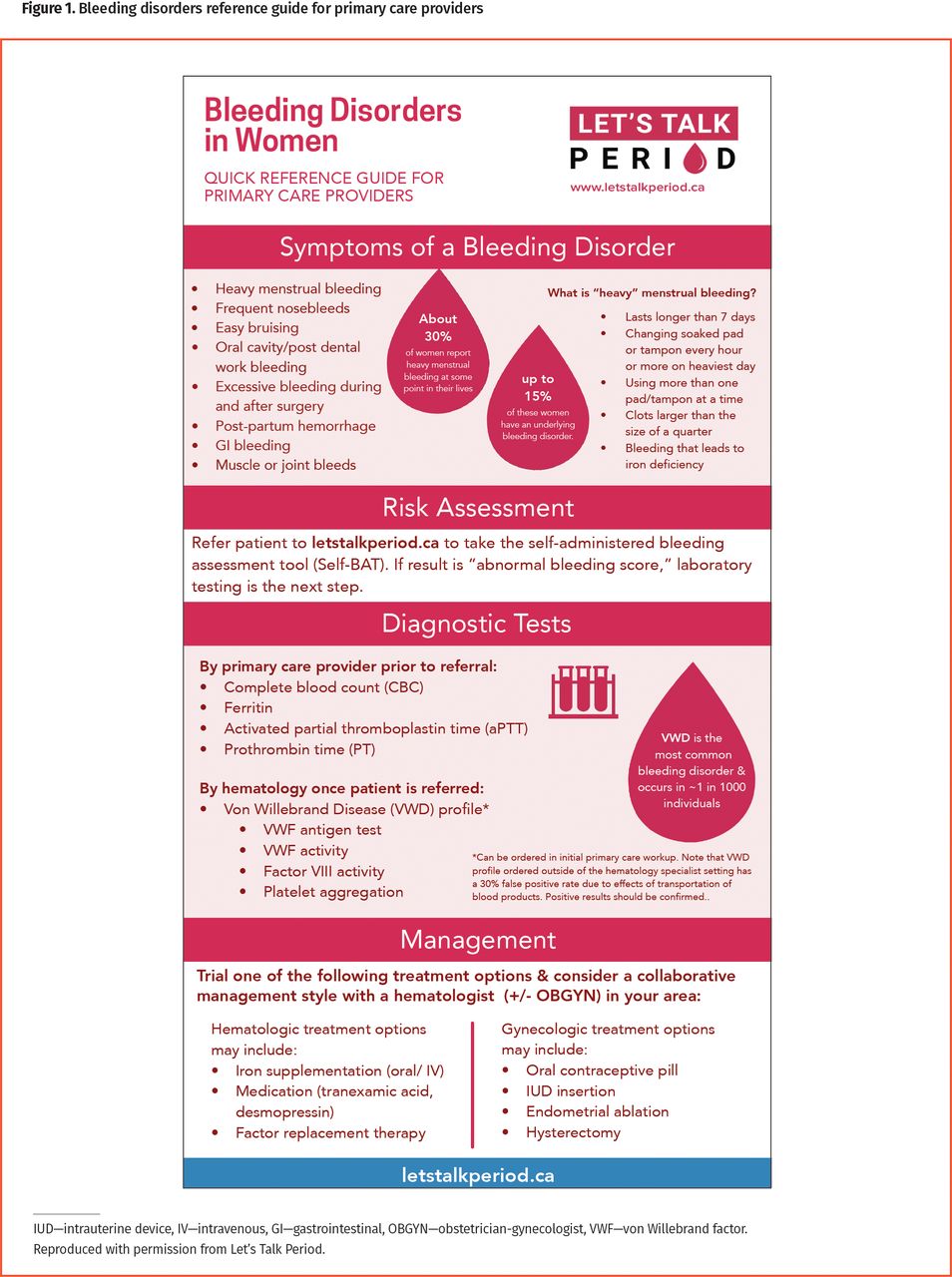
It is important that family physicians are equipped with the necessary resources and information to implement the Self-BAT as a screening tool, interpret bleeding scores, and use the Self-BAT to inform care and referral effectively.13 Therefore, we have introduced a resource (Figures 1 and 2; printable versions are available from CFPlus*) to teach primary care providers about the Self-BAT, including how it can be used for risk assessment, how to interpret its results, recommended diagnostic tests, appropriate management and referral, and clinical pearls for reviewing abnormal Self-BAT results. This tool is applicable in clinical practice when individuals present to primary care providers with an abnormal Self-BAT score or other bleeding symptoms that suggest an undiagnosed bleeding disorder may be present.

Bleeding disorders reference guide for primary care providers

Bleeding disorder clinical pearls
Case description
F.A. is a 22-year-old woman who sees her family physician after completing the online Let’s Talk Period Self-BAT. She did the assessment because she has had heavy menstrual periods and iron deficiency since menarche. She has a score of 6 (normal female range 0 to 5). Her family physician is not familiar with the Self-BAT and wants to know how the bleeding score will affect clinical management.
Sources of information
The poster tools and reference guide resources were created by synthesizing information from primary research sources and clinical review articles and by synthesizing formal data and qualitative feedback from 10 individuals (4 research staff, 2 nurses involved in the care of bleeding disorder patients, 1 hematologist, 1 family physician, and 2 medical students, all from Queen’s University in Kingston, Ont) who were interviewed to identify gaps in clinical practice in the fall of 2019.
Main message
Recommendations for management of a patient with an elevated Self-BAT score or other bleeding symptoms presenting to a primary care provider include reviewing the results of the Self-BAT to clarify relevant symptoms, performing initial diagnostic laboratory tests, and doing basic symptom management. Determining the threshold for referral to a hematologist is up to the primary care provider’s clinical judgment, but referral should be considered if the bleeding score is abnormal or if initial management options are ineffective.
Self-BAT review with patient. Since the Self-BAT was developed and validated as a patient-administered version of the health care professional–administered ISTH-BAT, either tool can be used in the clinical setting to review a patient’s bleeding symptoms.12,16,19 Both tools consider a score of 4 or more in males and 6 or more in females as abnormal, with higher scores indicating a greater likelihood of the presence of an inherited bleeding disorder.13 It is important to note that a normal bleeding score does not always rule out the presence of a bleeding disorder, especially in men and children who may not have had the opportunity to bleed. Clinical judgment plays an important role in decision making and thresholds for referral.
Diagnostic tests. Recommended initial laboratory tests include complete blood count, ferritin level, and activated partial thromboplastin time (aPTT) and prothrombin time.20 Activated partial thromboplastin time and prothrombin time tests can rule out factor deficiencies as the cause of bleeding; however, normal test results or an isolated, prolonged aPTT do not rule out VWD in a patient presenting with bleeding symptoms. Von Willebrand disease tests (ie, von Willebrand factor [VWF] antigen tests, platelet-dependent VWF function tests such as those measuring the binding of VWF to the gain-of-function mutant glycoprotein Ib fragment and those measuring factor VIII coagulant activity) can be ordered by initial primary care provider workup or by a hematologist, and they can confirm VWD. Depending on the laboratory, assays ordered in the community can have up to a 30% false-positive rate because of preanalytical variables (ie, the effect of delayed transport or testing and samples not being kept at the proper temperature).12,21 It is recommended to interpret a positive result with caution or to have results confirmed by a hematology clinic.20,22
Clinical pearls. During the process of reviewing Self-BAT results with patients, certain symptoms will need to be explored and managed. Helpful clinical pearls for each of the Self-BAT symptom categories are shown in Figure 2 and can assist in the referral process, as not all symptoms warrant evaluation by a hematologist or other specialist.
Bleeding disorder presentation may differ in pediatric versus adult populations. While a single symptom in an adult rarely justifies referral to a hematologist, single bleeding symptoms in pediatric patients—such as the presence of recurrent bruising, procedural bleeds, epistaxis, or heavy menstrual bleeding—may suggest an underlying bleeding disorder.
Management. There are many treatment options for a family physician to trial before or in tandem with a hematologist or obstetrician-gynecologist referral. Hematologic treatment options may include oral or intravenous iron supplementation, hemostatic medications such as tranexamic acid or desmopressin, or factor replacement therapy.20 Gynecologic management for heavy menstrual bleeding may include hormonal contraceptives, intrauterine device insertion, endometrial ablation, or sometimes hysterectomy.23-25
Case resolution
F.A.’s family physician reviews the results of her completed Self-BAT. Besides having menorrhagia and iron deficiency since menarche, F.A. also experiences epistaxis and easy bruising, and she had prolonged bleeding following dental extraction. After performing a more in-depth history, the family physician is unable to determine a known cause for the multiple bleeding symptoms. For example, the epistaxis from both nostrils has no seasonal variation and the patient is not on any medications that could potentially increase bleeding risk. The presence of multiple unexplained bleeding symptoms leads the physician to be suspicious of an inherited bleeding disorder. Basic blood work is ordered that confirms iron-deficiency anemia; prothrombin time is normal and aPTT is prolonged. Abnormal aPTT and the presence of bleeding symptoms prompt the physician to order a workup for VWD. The results come back positive and a diagnosis of VWD is made. To treat the bleeding symptoms, she prescribes and inserts a levonorgestrel intrauterine device with the goals of reducing bleeding and pain during menstruation and of lessening the need for iron supplementation. Additionally, she prescribes an oxymetazoline nasal spray for the management of epistaxis and tranexamic acid tablets for the management of bleeding episodes. A referral to a hematologist for long-term VWD management and education is made.
Conclusion
Knowing how to interpret a Self-BAT score is essential to facilitating diagnosis and informing treatment recommendations. An effective review of the Self-BAT score and bleeding symptoms with a patient can ensure that a thorough history and examination is completed and can allow the physician to make patient-centred health care decisions while informing appropriate referral to relevant specialists. The current underdiagnosis of bleeding disorders, particularly among women, has substantial preventable physical and psychological implications.9 Difficulty quantifying bleeding manifestations, lack of consensus surrounding nomenclature and diagnostic thresholds, and inappropriate referral to specialists all pose challenges to patient care. We hope that the clinical pearls and resources introduced here will support the integration of the Self-BAT into standard care for patients presenting with bleeding symptoms or elevated Self-BAT scores. The guide’s symptom-specific recommendations, initial diagnostic workups, symptom management, and clarification of hematology referral thresholds will allow primary care providers to better address the needs of individuals with inherited bleeding disorders and lessen the burden of disease through more effective interventions. Further research should evaluate the effectiveness of the reference tool in supporting the integration of the Self-BAT into patient management in clinical practice and should help address current gaps in bleeding disorder management.
Notes
Editor’s key points
▸ The self-administered bleeding assessment tool (Self-BAT) is a patient-friendly version of the International Society on Thrombosis and Haemostasis BAT that has been validated as a screening tool for inherited bleeding disorders.
▸ Scores of 4 or greater in males and of 6 or greater in females are considered abnormal, with positive scores suggesting the presence of an inherited bleeding disorder. However, normal scores do not always preclude bleeding disorders, especially in men and children, who may not have had the opportunity to bleed. Clinical judgment should be used when considering referral to a hematologist.
▸ Primary care providers should conduct a thorough review of the Self-BAT results with patients to ensure effective and timely treatment. The review should include clarification of relevant symptoms, appropriate laboratory tests, and patient education.
Footnotes
↵* Printable versions of Figures 1 and 2 are available from https://www.cfp.ca. Go to the full text of the article online and click on the CFPlus tab.
Contributors
Katie Yeung and Clare McGrath conceived of the idea for the manuscript, contributed to the literature review and interpretation, cowrote the initial draft of the manuscript, revised the manuscript, and prepared the final manuscript for submission. Dr Kelly Howse and Dr Paula James oversaw the project, provided data, and made substantial editorial revisions, including providing final approval of the manuscript.
Competing interests
None declared
This article is eligible for Mainpro+ certified Self-Learning credits. To earn credits, go to https://www.cfp.ca and click on the Mainpro+ link. This article has been peer reviewed.
Cet article se trouve aussi en français à la page 501.
- Copyright © 2022 the College of Family Physicians of Canada
References
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.