

Abstract
OBJECTIVE To determine an appropriate approach to managing prolactin-secreting adenomas of varying severity in pregnant women.
SOURCES OF INFORMATION MEDLINE was searched using the key words “hyperprolactinemia,” “prolactinoma,” “pregnancy,” and “management.” Experience from a multidisciplinary tertiary care centre was also reviewed. Recommendations are based on mostly levels II and III evidence.
MAIN MESSAGE With appropriate management, most women with hyperprolactinemia can achieve pregnancy. Although most women with prolactin-secreting adenomas during pregnancy need only careful observation, others might require medical treatment or even surgical evacuation. Ideally, such patients should be managed by multidisciplinary teams. In the absence of such teams, most pregnant women with small tumours can be managed safely by their primary physicians. Those with large tumours should be referred to specialists.
CONCLUSION Family physicians play an important role in managing women with prolactinomas during pregnancy. Knowledge of current approaches to management is crucial in determining when and how to refer these patients.
Prolactin-secreting adenomas are the most commonly encountered pituitary tumours in women of childbearing age.1 Hyperprolactinemia interferes with the hypothalamic-pituitary-ovarian axis at various levels and is responsible for about a third of all cases of female infertility.2 Although the true prevalence of hyperprolactinemia is difficult to establish, it is estimated that among women presenting with reproductive disorders, approximately 15% with anovulation and 43% with anovulation and galactorrhea have hyperpro-lactinemia.3 With adequate management, most women are expected to achieve successful pregnancies; however, managing prolactinomas during pregnancy poses a unique challenge.
When there is no dedicated multidisciplinary team, family physicians have an important role in managing these patients. This article focuses on the issues pertaining to management of prolactinomas during pregnancy. These issues are illustrated by 3 clinical cases of varying severity. The purpose of this article is to help family physicians provide high-quality care to most pregnant women with uncomplicated prolactinomas and identify patients who need to be referred to specialists.
Sources of information
MEDLINE was searched from January 1966 to May 2006 using the key words “hyperprolactinemia,” “prolactinoma,” “pregnancy,” and “management.” Most articles offered levels II and III evidence. The extensive experience of our multidisciplinary adult neuropituitary program constituted the main background information for the recommendations.
Effects of pregnancy on prolactinomas
The pituitary gland undergoes global hyperplasia during pregnancy. Growth begins within the first few weeks of pregnancy, and the gland expands to almost 1.2 cm in diameter during the immediate postpartum period.4–6 This increase in size is accompanied by a concomitant increase in size and population of lactotroph cells7 and a progressive increase in serum prolactin.8 The placental estrogen surge during pregnancy has been shown to induce the mitotic activity of lactotrophic cells as well as synthesis of prolactin.9 Tumour cells in patients with prolactinomas express estrogen receptors,10 thereby raising the logical concern about possible tumour enlargement during pregnancy.
The relationship between pregnancy and growth of prolactinomas was first identified in the early 1970s when it was noted that, in women who had previously been treated with ovulation-inducing agents or bromocriptine, pregnancy was associated with pituitary growth.11–14 Some of these patients subsequently developed visual defects that required surgery; other patients’ vision became normal spontaneously after parturition.11–14
Although managing patients with prolactinomas has been transformed by the introduction of new drugs, not enough safety data are available to recommend routine use of these drugs during pregnancy. As there have been no “classical” clinical trials, most of the evidence for management has been derived from observational studies and expert opinion, which has led to variability in management practices. The following case histories describe typical presentations of prolactinomas during pregnancy.
Managing microprolactinomas during pregnancy
Mrs Smith is 27 years old and was seen by her gynecologist for inability to conceive. Her initial screen results showed an elevated prolactin level of 64 μg/L (normal level is 2 to 15 μg/L). A subsequent magnetic resonance imaging scan confirmed the presence of a 5-mm pituitary adenoma. She was given bromocriptine, which normalized her menstruation as well as her prolactin level. She informed her family physician that she was pregnant and was not sure whether she should stop taking her bromocriptine.
Microprolactinomas (tumours <10 mm in diameter) tend to follow a benign course in nonpregnant patients. A 5-year prospective follow-up study15 of 30 women with untreated hyperprolactinemia associated with microadenomas showed that up to 35% of women resumed menses or had resolution of galactorrhea, and none developed visual loss or pituitary insufficiency. Serum prolactin levels became normal in 6 women and were reduced by more than 50% in about a third of the women.15 Long-term studies of women with untreated hyperprolactinemia have shown that the likelihood of progression from microprolactimoma to macroprolactinoma (tumours >10 mm) ranges from 0% to 12.5%.16–18 Risk of a clinically relevant increase in the size of a microprolactinoma during pregnancy is also quite small. Surveys of women with microprolactinomas during pregnancy have indicated that the risk of new neurologic sequelae (headaches, optic nerve compression, or stalk compression) ranges from 1.6% to 5.5%.19–21
A recent study22 followed 80 pregnancies in 56 women with microprolactinomas. During the 71 full-term pregnancies in this group, only 1 patient developed headaches (the headaches disappeared when bromocriptine was restarted), and 5 showed mild tumour growth on postpartum imaging.
No clinical trials have compared the outcomes of women with microprolactinomas treated pharmacologically with those not treated during pregnancy. This has led to variability in management practices. Most specialists discontinue dopamine agonist (DA) treatment upon confirmation of pregnancy; some prefer to continue DA treatment during pregnancy. The DA most widely used during pregnancy is bromocriptine, which is a semi-synthetic ergot alkaloid. Bromocriptine treatment leads to tumour shrinkage in approximately 90% of nonpregnant patients.23,24 A survey25 of more than 1400 pregnant women who took bromocriptine primarily during the first few weeks of pregnancy found no evidence of increased rates of abortion or congenital malformations.
Cabergoline is another ergot-derived DA whose higher affinity for D2 dopamine receptors results in a longer duration of action. Cabergoline is generally administered twice weekly and is better tolerated than bromocriptine.26 Experience with cabergoline during pregnancy is even more limited. A study of 226 women treated with cabergoline during pregnancy found no increase in fetal malformations, preterm delivery, ectopic pregnancy, or multiple-birth deliveries.27 Another newer agent is quinagolide, which is a non-ergot DA structurally similar to apomorphine. It is administered as a single daily dose. Once again there is limited experience with use of quinagolide during pregnancy. In a review of 176 pregnancies in which quinagolide was used (for an average of 37 days), 14% of the women had spontaneous abortions, 1 had a premature delivery, and 1 had an ectopic pregnancy.28 In another small study29 of 9 pregnancies, 2 patients were treated with quinagolide due to tumour enlargement and had no complications.29 Not enough information is available at this time to support routine use of either cabergoline or quinagolide during pregnancy.
Our practice (Figure 1) with patients such as Mrs Smith is to stop DA therapy once pregnancy is confirmed (level II evidence). We inform patients about the small risk of tumour enlargement and ask them to contact us if any unusual symptoms, such as headaches or visual problems, occur. Although the risk of tumour progression is small, it is not negligible. We obtain baseline Goldman visual field perimetry at the time of diagnosis and follow these patients every 2 months with clinical assessment and visual field perimetry during their pregnancies (level III evidence).
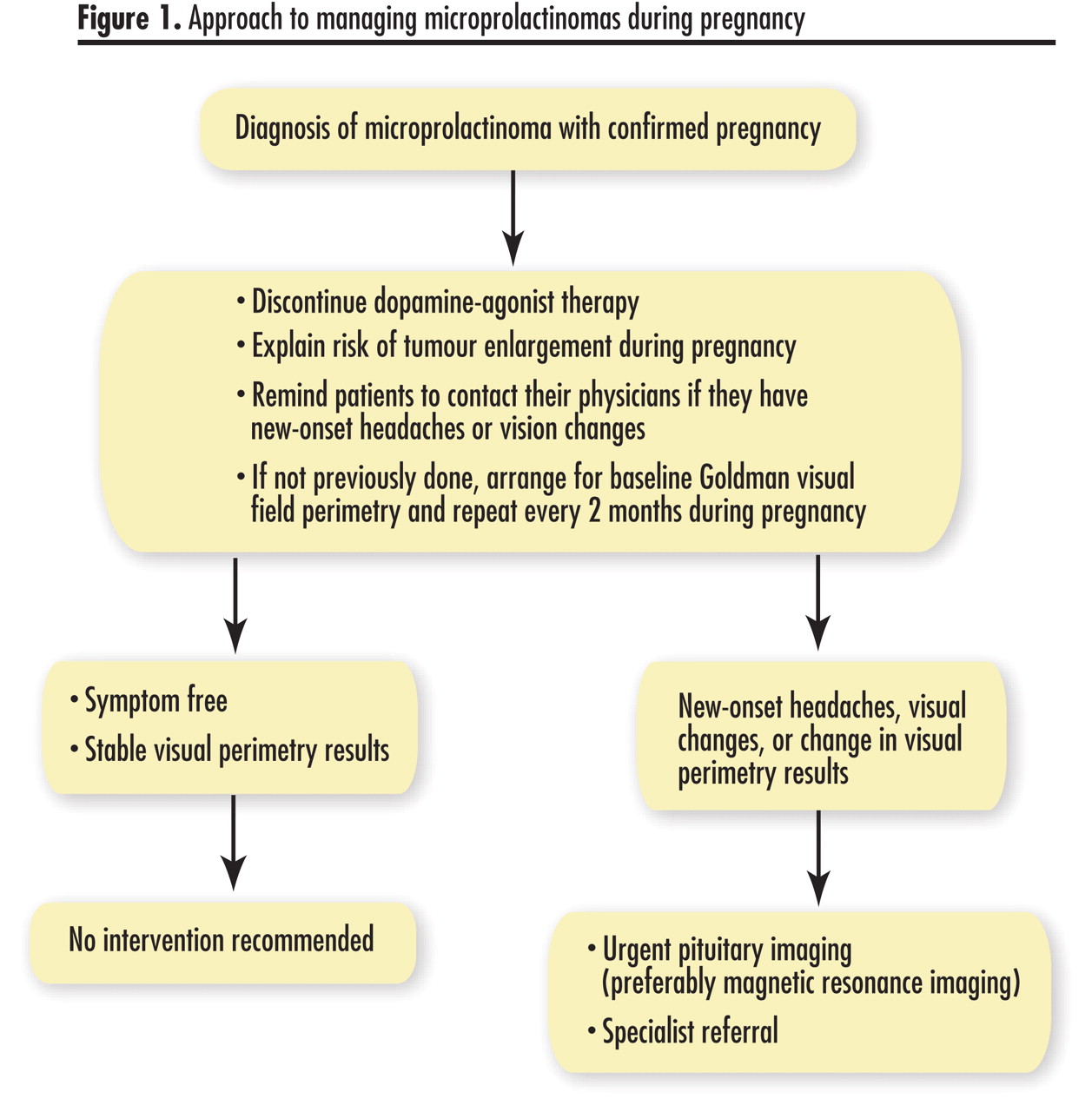
Approach to managing microprolactinomas during pregnancy
Despite the high degree of correlation between tumour volume and serum prolactin in nonpregnant patients, routine measurement of serum prolactin, as a marker of tumour growth, in pregnant patients is of little benefit because of the variability of physiologic hyperprolactinemia during pregnancy.30 New-onset headaches or visual field abnormalities should alert physicians to consider tumour enlargement and to arrange for urgent imaging of the pituitary. Computed tomography is unable to visualize the sellar and parasellar region properly, so MRI is the preferred imaging method. If substantial tumour growth is evident, immediate reinstitution of DA therapy is appropriate, and specialist referral is indicated.
In patients with uncomplicated pregnancies who were taking DA therapy before pregnancy and who do not wish to breastfeed, treatment can be restarted immediately after delivery. Although there is no evidence of any maternal risk with DA therapy when used in the context of prolactinoma, case reports31 have described acute myocardial infarction in women treated with bromocriptine for suppressing lactation. If women choose to breastfeed, an MRI scan should be done to ensure that tumour size is unchanged from baseline within 4 to 6 weeks of delivery (level III evidence).
Managing macroprolactinomas during pregnancy
Mrs Jones, a 33-year-old artist, had originally presented to her family physician with milky breast discharge about 6 years ago. Subsequent investigations revealed an elevated prolactin level of 752 μg/L. Pituitary MRI confirmed a 1.7-cm sellar lesion with suprasellar extension that was consistent with pituitary macroadenoma. Visual field testing revealed a defect in her left superior temporal field. She was started immediately on bromocriptine, and within 3 months, her serum prolactin level returned to normal, and her tumour shrank to 1.3 cm. Her visual field test results were normal. She has been under yearly surveillance at the local hospital, and her serum prolactin level has remained normal. Mrs Jones is now planning to get pregnant and wonders whether she should stop taking her bromocriptine.
Macroprolactinomas occur less frequently than microprolactinomas in women. Although it seems reasonable to assume that macroadenomas develop from microadenomas, large tumours are rarely found at autopsy, while small ones are common.32 It has been suggested that macroadenomas might in fact be an entirely separate disease because these large tumours shrink markedly with DA therapy,33 unlike microadenomas, and tend to be less vascular than microadenomas.34 Macroadenomas also behave differently during pregnancy and pose a much higher risk of adverse outcomes. A prospective survey of 56 pregnant women with macroprolactinomas revealed a 36% rate of adverse outcomes19: headaches (9%), headaches and visual impairment (25%), and diabetes insipidus (<1%). Subsequent studies have reported neurologic symptoms (13%)20 and visual impairment (75%)21 in women with macroprolactinomas during pregnancy.
From a family physician’s point of view, it is critical that women with macroprolactinomas be counseled appropriately about risk of tumour growth before they consider pregnancy. Such patients should be referred to specialists early on.
No randomized trial to date has compared various management strategies to reduce risk and improve outcomes for patients with macroprolactinomas during pregnancy. Management in these cases must be individualized, and patients should be closely monitored by their family physicians along with a team of endocrinologists and neurosurgeons.
Without definitive data, most physicians treat smaller macroadenomas (ones that do not abut the optic chiasm) as they would microadenomas. They discontinue DA therapy in these patients and follow them clinically with serial visual perimetry.22,35 As noted earlier, unexpected occurrences would demand urgent MRI. If evidence shows tumour enlargement, DA therapy should be started, and patients should be urgently referred to specialists. Large macroadenomas must be definitively treated before conception.35 Definitive treatments include either aggressive DA therapy to shrink the tumour or surgical evacuation of the bulk of the tumour. If tumours are DA-sensitive, patients could be maintained on DA therapy throughout pregnancy and informed that these drugs inhibit lactation. Although surgery would theoretically reduce the risk of tumour enlargement, there have been cases of massive tumour expansion during pregnancy even after surgery.36 Most specialists would keep such patients on DA therapy throughout pregnancy.
Our own approach is summarized in Figure 2. With smaller macroadenomas that do not abut the optic chiasm and those that have shrunk substantially in response to DA therapy, we discontinue therapy upon confirmation of pregnancy (level III evidence). We follow these patients throughout pregnancy with visual field tests every 2 months and ask them to report promptly persistent headaches or visual symptoms (level III evidence). For women with large tumours abutting the chiasm, we recommend definitive treatment before pregnancy. These patients receive a trial of DA therapy, and if the tumour shrinks, are allowed to proceed with pregnancy. They are maintained on DA therapy throughout pregnancy and are followed closely. When tumours are resistant to DA ther apy, we recommend surgery before conception.

{kind=link}
{kind=link}
Approach to managing microprolactinomas before pregnancy
Ms Brown, a 35-year-old nulliparous bartender who is 13 weeks pregnant, presented with frontal headaches that had been getting worse during the past 2 weeks. She was told 6 years ago that she had a prolactinoma and was given bromocriptine. She last saw the endocrinologist more than 3 years ago. She has been filling her prescription through her family physician and takes her bromocriptine intermittently. Her menstruation has always been irregular. In fact, she learned about her pregnancy only 4 weeks ago when she noticed she had gained some weight. She thinks she last took her bromocriptine about 3 months ago. Results of physical examination were unremarkable apart from bitemporal hemianopia on clinical visual field testing. An urgent MRI was requested. It showed a large (2.8 cm) lobulated sellar tumour compressing the optic chiasm. Her serum prolactin level was 3500 μg/L.
Enlarging prolactinomas during pregnancy are a serious challenge. This scenario represents a medical emergency, with high risk of irreversible vision loss or of pituitary insufficiency during the pregnancy. Family physicians’ role in managing such cases is limited, as patients must be referred immediately to specialists. Managing these tumours primarily consists of aggressive DA therapy to effect immediate and sustained tumour shrinkage. Most macroprolactinomas shrink with DA therapy24,37; maximum shrinkage occurs within 3 months. Nevertheless, such patients must be followed very closely with visual perimetry studies and, as necessary, MRIs because the tumours might be resistant to DA therapy.38
Emergency pituitary surgery during pregnancy is difficult and is associated with morbidity for mothers (eg, blood loss, incomplete evacuation, hypopituitarism) and fetuses (including a 1.5-fold increase in fetal loss during first trimester and a 5-fold increase during the second trimester).39 Clearly, surgery is a suboptimal last resort, and the situation emphasizes the need for planned proactive management of macroadenomas. Such careful management is key to excellent outcomes for mothers and babies.
Conclusion
Family physicians have an important role in diagnosing and managing prolactin-secreting adenomas during pregnancy. Outcomes with microprolactinomas can be excellent, and these small tumours can be managed safely by family physicians. Macroprolactinomas, however, have a higher risk of enlarging during pregnancy, and patients with macroprolactinomas should be encouraged to discuss management with their family physicians before conception. These patients should be referred to specialists.
Notes
EDITOR’S KEY POINTS
-
Hyperprolactinemia is the cause of a third of all cases of female infertility, yet with adequate management, most patients are able to achieve pregnancy.
-
Macroprolactinomas are more likely to enlarge during pregnancy than microprolactinomas are.
-
Pregnant women with microprolactinomas can usually be managed by family physicians with careful monitoring of symptoms and regular visual field testing.
-
Specialist care is generally required for women with macroprolactinomas who are planning pregnancy.
POINTS DE REPÈRE DU RÉDACTEUR
-
L’hyperprolactinémie cause le tiers des cas d’infertilité chez la femme. Pourtant, avec une prise en charge adéquate, la plupart des patientes peuvent devenir enceintes.
-
Les macroprolactinomes sont plus susceptibles de grossir durant la grossesse que le sont les microprolactinomes.
-
Les médecins de famille peuvent habituellement prendre en charge les femmes enceintes ayant un microprolactinome si la surveillance des symptômes est rigoureuse et s’il y a test visuel régulier du site.
-
Il faut généralement les soins d’un spécialiste pour les femmes qui ont un macroprolactinome et qui planifient une grossesse.
Footnotes
-
This article has been peer reviewed.
- Copyright© the College of Family Physicians of Canada