

Abstract
Objective To determine the relative effects of population size, FP and GP supply, and other specialist supply on chemistry and hematology test volumes (ie, number of tests performed).
Design Population-level analysis using secondary data from the Calgary Health Zone for 2004 to 2009.
Setting Calgary, Alta.
Main outcome measures The relative effects of population size, FP and GP supply, and other specialist supply on laboratory test use.
Results Population size was the strongest predictor of test volumes in a multivariate analysis. The FP and GP supply was significantly negatively correlated with chemistry test volume (partial r2 = 0.186, P = .045). There was a trend toward decreasing use of hematology tests with increasing FP and GP supply (partial r2 = 0.117, P = .119).
Conclusion The relationship between FP and GP supply and laboratory test use is complex, but increasing numbers of FPs do not necessarily indicate an increase in laboratory test use and might be associated with a decrease in test use when other factors are controlled for.
A 2010 Health Council of Canada report concluded that FPs are overusing diagnostic imaging and overprescribing medications.1 However, the relationship between FPs and resource use is more complex than this analysis would suggest. It is true that per capita health spending is positively correlated with the supply of physicians and hospital beds.2 The overall relationship between physician supply and laboratory test use has not been adequately explored. The first point to be made is that not all physicians order tests at the same rate. For example, increased test ordering has been reported in certain demographic groups including female physicians,3,4 physicians in urban practices,4 and physicians with increasing time since medical school graduation.5 Moreover, in teaching hospitals, a large proportion of the variation in laboratory test use might be attributable to house staff.6 A better understanding of the role of FPs in laboratory test use is critically important, as inappropriate laboratory testing might represent 10% to 50% of hospital laboratory workload.7 In fact, the rationalization of laboratory testing is one of the key challenges facing laboratory medicine.8 It is plausible that an increase in FP supply would result in lower per capita test use, as the primary care emphasis on prevention and care coordination might lead to fewer emergency department and urgent care clinic visits and less “defensive” ordering of laboratory tests. A similar relationship was reported for use of clinical resources: a higher proportion of primary care physicians was associated with decreased hospital admissions, emergency department visits, and surgeries.9
To further explore the possible effect of primary care physician supply on the ordering of laboratory tests, I examined the relationships among population size, physician supply, and laboratory test volumes during a 6-year period in Calgary, Alta. The demographic characteristics of Calgary make it particularly amenable to this type of analysis, as both the population size and the physician supply are rapidly changing and there remains a considerable segment of the population (estimated to be 250 000 people in 2010) that does not have access to FPs.10 Also, despite overall population growth, the population age stratification during the period in question remained relatively stable.
METHODS
Quarterly data on physician supply (FPs and GPs, and other specialists) for the Calgary Health Zone from 2004 to 2009 were obtained from the physician supply reports of the College of Physicians and Surgeons of Alberta.11–13 Quarterly laboratory test volumes for the same period were obtained from Calgary Laboratory Services, the sole provider of laboratory services for the approximately 1.3 million residents of the Calgary Health Region. Data were analyzed separately for chemistry and hematology test volumes. Population estimates for the Calgary Economic Region were obtained from the Calgary Economic Development commission.14 Yearly population estimates were interpolated to provide quarterly estimates. The physician supply data are considered to be complete, as they are based on actual physician registration with the College of Physicians and Surgeons of Alberta. Likewise, essentially all laboratory tests (publicly and privately funded) in Calgary are performed by the Calgary Laboratory Services, making it highly likely that the test volume data are complete. Population estimates were based on the Calgary Economic Region rather than the Calgary Health Zone, but these geographic regions are highly similar. The raw data used in the analyses are given in Table 1. The relative effects of population size, FP and GP supply, and other specialist supply on laboratory test use were determined using multiple linear regression, with test volume as the dependent variable. Analyses were conducted using SPSS, version 15 for Windows.
Number of FPs and GPs, number of other specialists, total population, and laboratory test volumes for the Calgary Health Zone from 2004 to 2009, listed by quarter
RESULTS
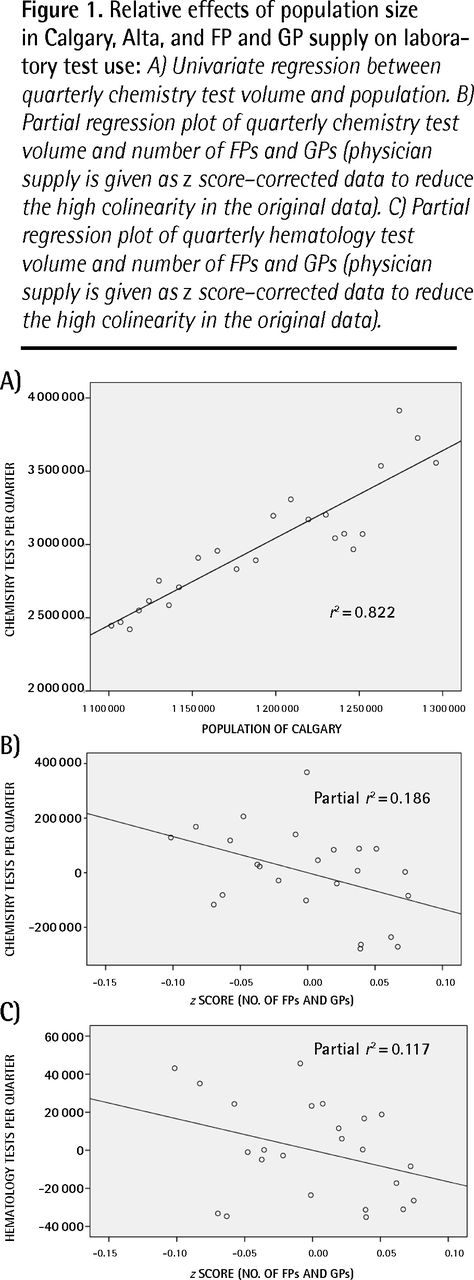
Population size, FP and GP supply, and other specialist supply were associated with increased use of both chemistry and hematology testing. The strongest relationship was between population size and test volumes. Representative of this, the relationship between population size and chemistry test volume is given in Figure 1A. However, population size, FP and GP supply, and other specialist supply are themselves highly correlated. To control for this, I performed a multiple linear regression with test volume as the dependent variable and population size, FP and GP supply, and other specialist supply as the independent variables. The resulting partial regressions provide estimates of the relative contribution of each of these variables. In this model, the strongest predictor of test volumes for both chemistry and hematology tests was population size (Table 2), which explained approximately 42% of the variation in chemistry test volume and 32% of the variation in hematology test volume. Increased FP and GP supply was associated with decreased test use, explaining approximately 18% of the variance in chemistry test volume (Figure 1B, Table 2) and 12% of the variance in hematology test volumes (Figure 1C, Table 2). This relationship was statistically significant for chemistry tests (P = .045) but nonsignificant for hematology tests (P = .119). Other specialist supply showed nonsignificant positive relationships with increased test volume (P = .303 and P = .446; Table 2).

{kind=link}
Relative effects of population size in Calgary, Alta, and FP and GP supply on laboratory test use: A) Univariate regression between quarterly chemistry test volume and population. B) Partial regression plot of quarterly chemistry test volume and number of FPs and GPs (physician supply is given as z score–corrected data to reduce the high colinearity in the original data). C) Partial regression plot of quarterly hematology test volume and number of FPs and GPs (physician supply is given as z score–corrected data to reduce the high colinearity in the original data).
Partial correlation coefficients (multiple linear regression) for laboratory test use in Calgary, Alta, and population size, FP and GP supply, and other specialist supply
DISCUSSION
In this study I have presented a population-level analysis of the correlates of physician supply and population size with laboratory test volume. Owing to the nature of the available data, it was not possible to account for the possible effects of differences in access to FPs by patient and disease type. In this analysis, population size was the greatest predictor of laboratory test use; the number of FPs and GPs and other specialists in Calgary was a poorer predictor of laboratory test use. I found evidence to suggest that increasing FP and GP supply might actually decrease laboratory test use when other variables are controlled for. Although the association was statistically significant for chemistry test volume and FP and GP supply, the association was not significant for hematology test volume and FP and GP supply. This might be owing to the relatively small sample sizes or might be related to the observation that per capita chemistry test use has increased at a faster rate than per capita hematology test use (Table 1).
A possible explanation for the association between laboratory test use and FP and GP supply is that patients with access to FPs might rely less on emergency departments and urgent care clinics and so might have fewer defensive investigations. This finding might appear to be at odds with the 2010 report by the Health Council of Canada that concluded there is overuse of prescription drugs and diagnostic imaging by Canadian FPs.1 However, a question not addressed in the Health Council of Canada report is whether care provided by FPs results in more or less overall use of health care resources than care provided in other settings. There are serious imbalances in the physician supply in Canada, with shortages in rural areas in particular.15,16 The resulting barriers to care might result in less preventive care, such as childhood immunizations, where fewer physicians are practising.17 In addition to the direct effects on patients from a lack of access to care, a shortage of primary care physicians in a given area might also lead to increased laboratory test use.
Finally, it should be noted that a reduction in laboratory test volumes does not necessarily imply more appropriate testing. It is possible (but not likely) that patients visiting FPs are receiving an inadequate number of laboratory tests. This last point will require more detailed examination of individual test appropriateness according to physician and patient demographic groups.
Conclusion
Although population size was the strongest predictor of overall laboratory test use, increasing primary care physician supply might actually lead to decreased test use.
Notes
EDITOR’S KEY POINTS
-
Although population size was the strongest predictor of overall laboratory test use, increasing primary care physician supply might actually lead to decreased test use. A possible explanation for the association between laboratory test use and FP and GP supply is that patients with access to FPs might rely less on emergency departments and urgent care clinics and so might have fewer defensive investigations.
-
Although there was a statistically significant association between chemistry test volume and FP and GP supply (P = .045), the association between hematology test volume and FP and GP supply was not significant (P = .119).
POINTS DE REPÈRE DU RÉDACTEUR
-
Même si la taille de la population était le meilleur indice de l’utilisation globale des examens de laboratoire, la disponibilité d’un plus grand nombre de médecins de première ligne pourrait même entraîner une diminution des demandes d’examens. Cette association entre la disponibilité de MF et d’OP l’utilisation des examens de laboratoire pourrait s’expliquer par le fait que les patients qui ont accès à un MF comptent moins sur les départements d’urgence et sur les cliniques de soins d’urgence, si bien qu’ils auraient moins d’investigation de type défensif.
-
Même s’il existe une association statistiquement significative entre le volume des examens chimiques et la disponibilité de MF et d’OP (P = ,045), l’association entre le nombre d’examens hématologiques et la disponibilité de MF et d’OP n’était pas significative (P = ,119).
Footnotes
-
This article has been peer reviewed.
-
Cet article a fait l’objet d’une révision par des pairs.
-
Competing interests
None declared
- Copyright© the College of Family Physicians of Canada