

Abstract
Objective To systematically review the literature and provide an update and integration of existing peer-reviewed guidelines with recent systematic reviews and with primary studies related to the early recognition and management of lung cancer in primary care.
Data sources MEDLINE and EMBASE were searched for relevant articles. The quality of the evidence to support existing guideline recommendations, and the consistency of recommendations with updated evidence, were assessed. Applicability in a Canadian primary care setting was also evaluated.
Study selection All studies that explored signs or symptoms of or risk factors for lung cancer in the primary care setting were included. All diagnostic studies in which symptomatic primary care patients underwent 1 or more investigations were also searched.
Synthesis Recommendations were consistent among guidelines despite a paucity of supporting evidence. Updated evidence provided further support for the recommendations. Recommendations for identifying signs and symptoms of lung cancer presenting in primary care and for initial management can be adopted and applied within a Canadian primary care setting.
Conclusion This updated review of recommendations might help promote evidence-based practice and, ultimately, more timely management and improved prognosis for lung cancer patients. It might also assist in the development of lung cancer diagnostic assessment programs.
Lung cancer is the most common cause of cancer death in Canada.1 Tobacco use is the primary cause of lung cancer, accounting for an estimated 86% of cases.2 The chance of surviving lung cancer in Canada is low, with a 5-year survival rate for all types and all stages combined of 13% for men and 19% for women.1 Lung cancers are most frequently diagnosed at a late stage, when prognosis is very poor. Delays in the diagnosis of lung cancer have, in part, been found to be associated with physicians failing to recognize early signs and symptoms.3,4 This could be owing to both physicians and patients attributing the often common, atypical, or nonspecific signs and symptoms of lung cancer to other benign diseases.3–5
A working group was formed to develop an updated comprehensive consensus document for primary care providers that would assist them in the early identification and management of patients with lung cancers. The systematic review presented here formed the basis of a companion guideline, and investigated what signs, symptoms, and other clinical features of patients who present in primary care are predictive of lung cancer.6,7 This updated review of the literature is intended to promote evidence-based practice and, ultimately, more timely management and improved prognosis of lung cancer patients.
DATA SOURCES
This systematic review was initiated by the Cancer Care Ontario Provincial Primary Care and Cancer Network in collaboration with the Program in Evidence-based Care. A working group was assembled consisting of 9 members including 5 FPs (M.E.D., S.Y., M.A., P.B., C.L.), 1 medical oncologist (A.R.), 1 respirologist (R.S.), 1 radiation oncologist (Y.U.), 1 thoracic surgeon (R.Z.), and 1 methodologist (E.T.V.). The specific objectives of this initiative were to update and integrate existing peer-reviewed evidence-based guidelines with recent systematic reviews and primary studies related to signs, symptoms, and other clinical features predictive of lung cancer; risk factors for lung cancer; and the diagnostic accuracy of early investigations for lung cancer. The final guideline was developed using the methods of practice guideline development cycle.8 An environmental scan was initially conducted (March 5 to 8, 2010). The 2009 guidelines from the New Zealand Guidelines Group (NZGG) and the 2005 guidelines from the National Institute for Health and Care Excellence (NICE) were chosen a priori as baseline documents for the development of the current updated systematic review.9,10 These guidelines were considered to be of high quality, comprehensive, recent, and relevant to this topic.9,10 Updated literature searches of the NZGG 2009 or NICE 2005 systematic reviews were completed. Additional relevant guidelines, systematic reviews, and prospective and retrospective studies were selected and evaluated.
Literature search strategy
The search strategies from NZGG 2009 and NICE 2005 were kindly provided to us.9,10 An updated search since the NZGG 2009 publication using MEDLINE (Ovid, August 2007 to week 3 of February 2010) and EMBASE (Ovid, 2007 to week 7 of 2010) was performed using the NZGG 2009 literature search strategy for the diagnostic accuracy of signs, symptoms, and investigations.10 Because it was not completed in the NZGG 2009 systematic review, an updated search of lung cancer risk factors since the NICE 2005 publication of MEDLINE (Ovid, June 2004 to week 3 of February 2010) and EMBASE (Ovid, 2004 to week 8 of 2010) was conducted using the NICE 2005 search strategies.9,10 A second literature search update of all strategies for literature available to June 27, 2011, was performed. The detailed search strategies are available upon request.
Study selection
Guidelines and systematic reviews were included if they addressed at least 1 of our objectives. They were also included if they provided different recommendations than or were not cited in the NZGG 2009 or NICE 2005 guidelines.9,10
All prospective or retrospective cohort or case-control studies that explored signs and symptoms of or risk factors for lung cancer in the primary care setting were included. All diagnostic studies in which symptomatic primary care patients underwent 1 or more investigations including complete blood count, chest x-ray scan, spirometry, sputum cytology, and computed tomography (CT) chest scan were also searched. Studies conducted in secondary care settings were included when limited evidence was available from primary care. Screening studies of asymptomatic patients were excluded.
Publications in a language other than English were not eligible owing to a lack of funding for translation. Non-systematic reviews, abstracts, case reports, letters, editorials, and commentaries were excluded.
There was considerable heterogeneity among studies; therefore, data were not pooled.
Quality appraisal of evidence-based guidelines and systematic review
The AGREE II (Appraisal of Guidelines Research and Evaluation) tool was used by 3 independent methodologists to evaluate the quality of the evidence-based guidelines.11,12 Using the AGREE II tool, only clinical practice guidelines in which the objective of the guideline was specifically described and which included a review of the evidence were evaluated.11,12 The AMSTAR (Assessment of Multiple Systematic Reviews) tool was used to assess the quality of the 1 systematic review.13
SYNTHESIS
Literature search results
During the initial environmental scan, 6 guidelines in addition to the NICE 2005 and NZGG 2009 guidelines were identified.4,9,10,14–18 Of 12 013 articles identified in the updated literature search, 168 were deemed relevant for a full article review. Of these, 12 articles not included in the NICE 2005 or NZGG 2009 systematic review met the inclusion criteria and were retained (Figure 1).19–30
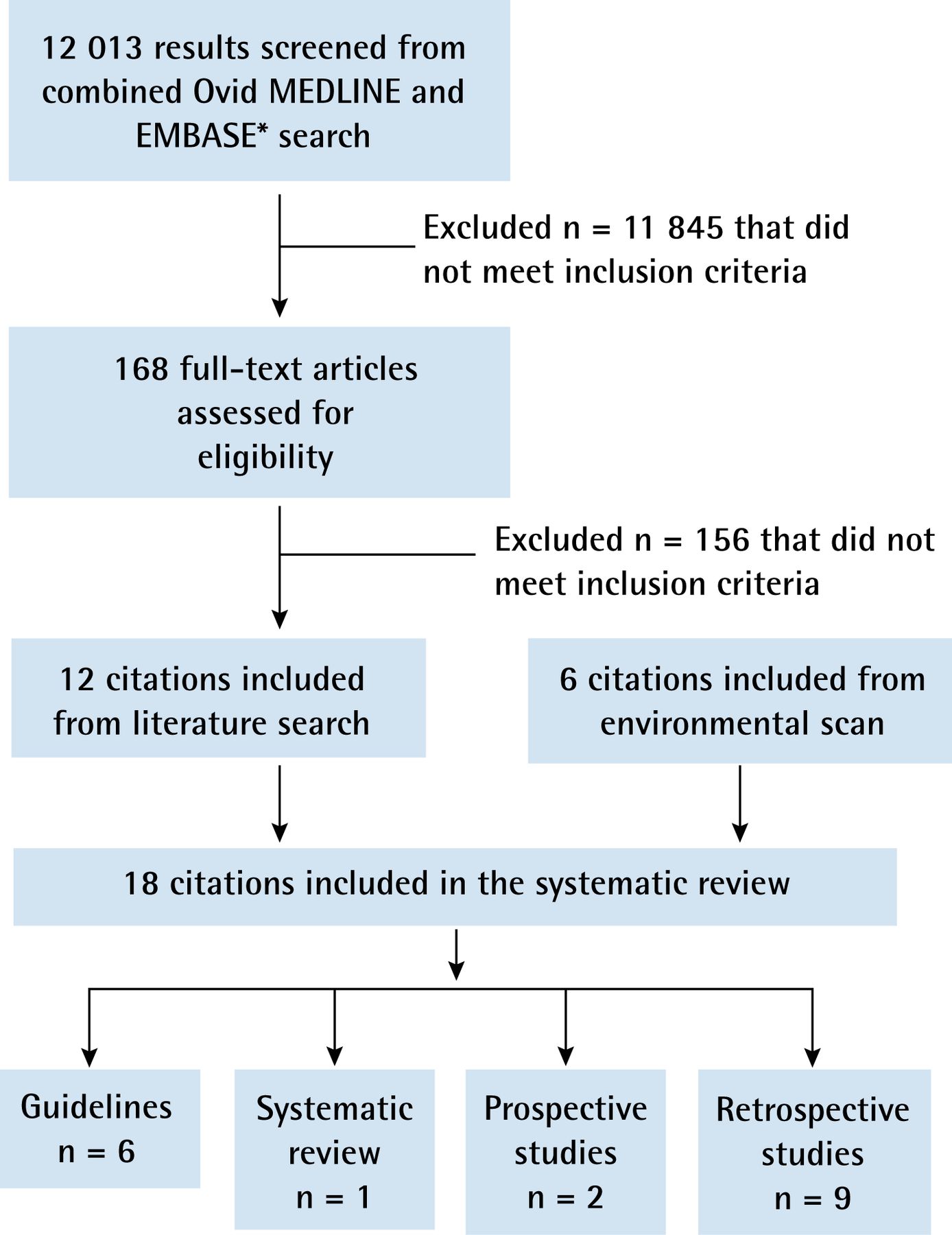
{kind=link}
Results of the literature search
*The online search strategy is available from the authors upon request.
The quality of the guidelines from NICE 2005, NZGG 2009, the Australian National Health and Medical Research Council, the Scottish Intercollegiate Guidelines Network (SIGN), and the American College of Chest Physicians (ACCP) was assessed using the AGREE II instrument (Table 1).4,9,10,14–18
Results of AGREE II tool quality rating of evidence-based guidelines
Summaries of the recommendations, the supporting evidence, and the rating of the evidence to support the recommendations are provided in Table 2.4,9,10,14–18,31,32 Details of the quality of the guidelines that were included in the systematic review are provided below.
Summary of guideline recommendations, literature review, and supporting evidence
The systematic review for signs and symptoms of lung cancer conducted by NICE in 2005 included 3 guidelines, only 1 of which provided a table of common signs and symptoms based on evidence from case series.9 These were not described in detail. Nine additional studies were included in the NICE 2005 systematic review. Data from only 2 of the 9 studies were collected from primary care records. The systematic review conducted by NICE in 2005 also included 1 systematic review with meta-analyses comparing the diagnostic accuracy of cytology, bronchoscopy, transthoracic needle aspirate, or biopsy.9 As well, 3 primary studies were included: 2 regarding chest radiography and 1 regarding bloodwork. The link between the evidence and the recommendations was not always clear.9 They noted that the literature lacked evidence to adequately address the research questions, especially within the context of primary care.
The updated literature search since NICE 2005 by NZGG 2009 for signs and symptoms associated with lung cancer included a case-control study by Hamilton et al from 2005 and a case-series study by Jones et al from 2007.33,34 In their updated systematic review for diagnostic investigations, NZGG identified an additional systematic review and 2 primary studies that provided further information on complete blood count, chest x-ray scans, spirometry, and sputum cytology.31,33,35
The ACCP published a series of evidence-based clinical practice guidelines for the management of patients with lung cancer. Four of these guidelines were included because they addressed at least 1 of the research questions.4,14–16 The ACCP guidelines did not provide lists or details of included studies and did not assess their quality. However, each of the recommendations was followed by a grading of the supporting evidence.4,14–16 A 2006 study by Kvale was included in the first edition of the ACCP clinical practice guidelines.15 Kvale focused on the management of cough associated with lung tumours; although MEDLINE was searched, only 2 terms were listed: cough and lung neoplasms.15 Studies by Spiro et al,4 Gould et al,14 and Rivera and Mehta16 were included in the second addition of the ACCP clinical practice guidelines. Spiro et al conducted a systematic review of the initial symptoms and signs of lung cancer, as well as the symptoms, signs, and laboratory tests that could be used in a standardized evaluation for systemic metastases and paraneoplastic syndromes associated with lung cancer.4 The search terms in MEDLINE and the inclusion and exclusion criteria were not outlined in the article.4 Gould et al performed a systematic review on the diagnosis and management of patients with pulmonary nodules, which did not distinguish between screen-detected nodules and nodules that were detected incidentally.14 Rivera and Mehta looked at 17 studies on sputum cytology.16 Rivera and Mehta and Gould et al searched more than 1 database and included their research questions, as well as their inclusion and exclusion criteria.14,16
Two additional guidelines were developed by SIGN in 2005 and the Australian National Health and Medical Research Council in 2004.17,18 The SIGN 2005 guidelines included evidence summaries from their systematic review with each of their recommendations, and also included a grading of the strength of the evidence for each recommendation.18 They provided their search strategies for MEDLINE, but their inclusion and exclusion criteria were not clearly defined. This guideline addressed the management of patients with lung cancer, including 4 studies on CT scans. As a result, studies completed in a primary care setting were not a priority. The Australian guidelines covered a broad spectrum of care for patients with lung cancer, from prevention and diagnosis to management.17 Studies were not selected on the basis of whether they were relevant to the primary care setting. The authors did not include their search strategy or their inclusion or exclusion criteria. They provided the strength of the evidence to support their recommendations, as well as the citations for each recommendation.
A systematic review by Shapley et al from 2010 was included in the updated literature search since the NZGG 2009 search.30 This systematic review scored well, with 8 of the 11 items meeting the AMSTAR criteria. The authors did not provide all excluded studies and did not assess the likelihood of publication bias. Although Shapley et al provided a conflict of interest statement, such statements were not acknowledged for the included studies. Shapley et al included studies that had positive predictive values of 5% or more for any sign or symptom, as well as studies with positive predictive values less than of 5% for the same sign or symptom.30 The 2 articles cited for lung cancer were already referenced in the NZGG 2009 guideline.33,34
Of the 11 primary studies published since the NZGG 2009, 9 had retrospective designs.19–29 Details of these studies are provided in Table 3. None of the studies was performed in a primary care setting. Nine of the studies looked at signs, symptoms, and risk factors.19–21,24–29 Only 2 primary studies provided information on the diagnostic accuracy of investigations for lung cancer.22,23 Both of these studies included patients with and without lung cancer and were blinded to the diagnostic results.
Primary studies and results from updated literature review
DISCUSSION
Owing to a paucity of evidence in the primary care setting for the diagnostic accuracy of signs, symptoms, and risk factors associated with lung cancer, definitive conclusions could not be derived for the recognition of lung cancer in patients presenting in primary care. However, owing to the consistency among systematic reviews, the working group agreed with the signs and symptoms of lung cancer listed in the NICE 2005 and NZGG 2009 guidelines, which included superior vena cava obstruction, stridor, hemoptysis, finger clubbing, enlarged lymph nodes, persistent or unexplained cough, unexplained weight loss, dyspnea, chest or shoulder pain, hoarseness, dysphagia, and abnormal chest x-ray findings.9,10 Patients might also present with signs and symptoms of metastases or paraneoplastic syndromes.4
Our literature review did not provide evidence for additional risk factors associated with lung cancer beyond those listed in the NICE 2005 or NZGG 2009 guidelines.9,10 In addition, no evidence was found to challenge and remove any of the risk factors listed. The risk factors for lung cancer include current or previous smoking, passive exposure to tobacco smoke, chronic obstructive pulmonary disease, previous exposure to asbestos, and a history of cancer (especially head and neck cancer). Other risk factors might include occupational exposure to dust or microscopic particles (eg, wood dust, silica), silicosis or tuberculosis, family history of cancer, and exposure to known carcinogens (eg, radon, chromium, nickel).
Based on the interpretation of the evidence for diagnostic tests, a chest x-ray scan should be ordered as a preliminary investigation for signs or symptoms of lung cancer. There is little evidence to support CT chest scan as an initial investigation. Sputum cytology should not be used as a primary investigation for lung cancer. Further investigation or referral is warranted if there is a suspicion of lung cancer despite a negative chest x-ray scan finding.
Limitations
The current literature search was an update of the searches completed for the NICE and NZGG guidelines, and we trusted that the original searches were equally as extensive and that relevant articles were not missed. This review is limited to only those studies published in English. The consistency of results seen among the primary studies and systematic reviews provides some reassurance that irretrievable information is unlikely to show contradicting evidence.
We were limited by the number of rigorous prospective studies that assessed signs, symptoms, risk factors, and initial investigations for patients presenting with undiagnosed lung cancer, especially in primary care. Most of the evidence supporting existing guidelines and systematic reviews came from case-control studies, case-series studies, and consensus based on clinical experience. Furthermore, some of the systematic reviews of this evidence did not provide search strategies, study inclusion or exclusion criteria, study details, or evaluation of the quality of the studies included.
As electronic medical records in primary care practices become more widely used, opportunities for rigorous large-sample prospective studies exploring the presentation of clinical features and initial investigations of cancer presenting in primary care should become increasingly more feasible.
Conclusion
Early detection of lung cancer is critical for improving survival. While some presenting symptoms might be vague and imprecise, delays in diagnosis might be avoided if patients presenting with suspicious signs and symptoms, especially in the presence of risk factors, receive timely chest x-ray scans and, where warranted, further investigation or referral. This updated review of recommendations might help promote evidence-based practice and, ultimately, more timely management and improved prognosis of lung cancer patients. It might also assist in the development of lung cancer diagnostic assessment programs.
Notes
EDITOR’S KEY POINTS
-
Lung cancer is the leading cause of cancer death in Canada. It is frequently diagnosed at a late stage, when prognosis is very poor. Delays in diagnosis have been associated, in part, with delays in recognizing symptoms. For FPs and other primary care providers it can be difficult to distinguish early presentation of lung cancer from other benign conditions.
-
This systematic review found the following signs and symptoms to be predictive of lung cancer: superior vena cava obstruction, stridor, hemoptysis, finger clubbing, enlarged lymph nodes, persistent or unexplained cough, unexplained weight loss, dyspnea, chest or shoulder pain, hoarseness, dysphagia, and abnormal chest x-ray findings. Risk factors for lung cancer include current or previous smoking, passive exposure to tobacco smoke, chronic obstructive pulmonary disease, exposure to asbestos, and history of cancer (especially head and neck cancer).
-
A chest x-ray scan should be the preliminary investigation for signs or symptoms of lung cancer. There is little evidence to support computed tomography chest scan as an initial investigation, and sputum cytology should not be used as a primary investigation. Further investigation or referral is warranted if there is a suspicion of lung cancer despite a negative chest x-ray scan finding.
POINTS DE REPÈRE DU RÉDACTEUR
-
Au Canada, le cancer pulmonaire est la principale cause de mortalité due au cancer. Ce cancer est souvent diagnostiqué à un stade avancé, son pronostic étant alors très mauvais. Ce diagnostic trop tardif a souvent été attribué en partie au fait que les symptômes n’étaient pas reconnus assez tôt. Pour les MF comme pour les autres soignants de première ligne, il peut être difficile de distinguer les symptômes précoces d’un cancer pulmonaire de ceux d’une autre affection bénigne.
-
D’après cette revue systématique, les signes et les symptômes suivants sont prédictifs d’un cancer pulmonaire: obstruction de la veine cave supérieure, stridor, hémoptysie, hippocratisme digital, hypertrophie ganglionnaire, toux persistante ou inexpliquée, amaigrissement inexpliqué, dyspnée, douleur au thorax ou à l’épaule, voix rauque, dysphagie et radiographie pulmonaire anormale. Les facteurs de risque du cancer pulmonaire incluent le tabagisme antérieur ou actuel, l’exposition passive à la fumée du tabac, la maladie pulmonaire obstructive, l’exposition à l’amiante et des antécédents de cancer, plus particulièrement au niveau de la tête et du cou.
-
Une radiographie du thorax devrait être l’examen préliminaire en présence de signes ou de symptômes de cancer pulmonaire. Il y a peu de données indiquant qu’une tomodensitométrie thoracique devrait être utilisée initialement; la cytologie des expectorations ne devrait pas non plus être utilisée comme premier examen. Il y a indication d’examens additionnels ou d’une consultation si on soupçonne un cancer pulmonaire, même en présence d’une radiographie pulmonaire négative.
Footnotes
-
This article has been peer reviewed.
-
Cet article a fait l’objet d’une révision par des pairs.
-
Contributors
All authors contributed to the literature review and interpretation, and to preparing the manuscript for submission.
-
Competing interests
None declared
- Copyright© the College of Family Physicians of Canada
References
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.
- 31.
- 32.
- 33.
- 34.
- 35.