

Heterotopic pregnancy (HP) is defined as multiple gestations at 2 or more implantation sites. Heterotopic pregnancy might include 2 ectopic pregnancies, but more commonly one of the pregnancies is intrauterine.1,2 Heterotopic pregnancy is more common with the use of assisted reproductive techniques (ART), with an estimated incidence of up to 1 in 100 in pregnancies using ART. However, it is rare in spontaneous conceptions, with an estimated prevalence of 1 in 30 000.3–6 Owing to the increased use of ART in the general population, estimates of the overall prevalence of HP in all pregnancies has been as high as 1 in 2600.3,7,8
In addition to the use of ART, risk factors include a history of ectopic pregnancy, pelvic inflammatory disease (PID), abdominal adhesions, reconstructive tubal surgery, and salpingectomy.1,2,9 The most common site of ectopic gestation is the fallopian tube (95% to 97%). Other sites include the cervix, ovary, and abdomen.3
Seventy percent of HPs are diagnosed between 5 and 8 weeks’ gestation, 20% between 9 and 11 weeks, and less than 10% after 11 weeks.10 Presenting signs and symptoms are nonspecific and might include abdominal pain, an adnexal mass, peritoneal irritation, and vaginal bleeding, as well as acute chest pain radiating to the shoulder.2,11,12 Heterotopic pregnancy carries a considerable risk of maternal morbidity and mortality owing to the risk of rupture of the ectopic pregnancy. Up to 33% of patients might initially present with hemodynamic instability.9 Therefore, prompt recognition in family medicine and acute care settings is crucial.
Case description
A 33-year-old woman (gravida 6, para 5) at 7 weeks’ gestation presents to the emergency department with a 5-hour history of severe abdominal pain and nausea without vaginal symptoms. This pregnancy was spontaneously conceived. She has a remote history of treated syphilis but no previous intra-abdominal or pelvic surgeries, gonorrhea, chlamydia, or PID. She takes prenatal vitamins, and her social history is unremarkable.
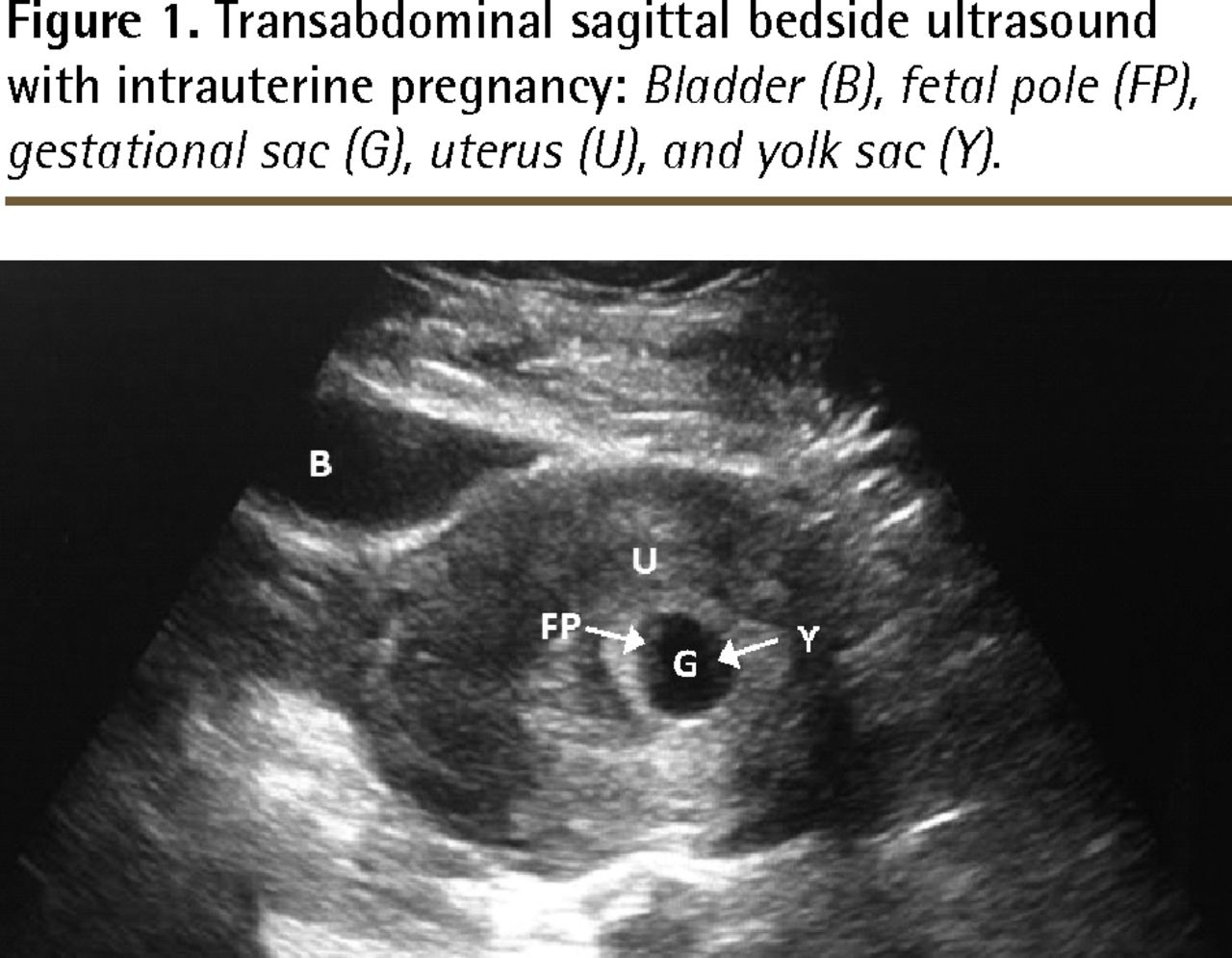
On examination, she is hemodynamically stable and afebrile. She has rebound tenderness in the suprapubic region, cervical motion tenderness, and a closed os with blood in the posterior vaginal fornix without purulent discharge. Bedside ultrasound shows a live intrauterine pregnancy (IUP) without free fluid (Figure 1), and her β–human chorionic gonadotropin (β-hCG) level is 52 096 IU/L; both investigations are appropriate for a 7-week gestational age. Examination findings are normal for complete blood count, liver function, electrolyte and amylase levels, and urinalysis. Cervical cultures are sent for testing and results are later found to be negative.
{kind=link}
Transabdominal sagittal bedside ultrasound with intrauterine pregnancy: Bladder (B), fetal pole (FP), gestational sac (G), uterus (U), and yolk sac (Y).
An urgent radiology obstetric ultrasound shows a definite HP, with an intrauterine gestational sac corresponding to a 7-week gestational age and ectopic pregnancy in the right adnexa with a fetal heartbeat.
Differential diagnosis
Heterotopic pregnancy is a rare but potentially fatal condition. A high level of clinical suspicion must be maintained and treatment must be prompt. The differential diagnoses for severe early pregnancy abdominal pain include miscarriage and ectopic pregnancy, as well as nonobstetric causes (Table 1).1
Differential diagnosis of nonobstetric causes of acute abdominal pain in pregnancy
Investigations
In suspected cases of HP, laboratory investigations should include complete blood count, measurement of electrolyte levels, urinalysis, sexually transmitted infection screening, and blood group and antibody screening (Rh status is imperative in any pregnancy) for potential volume replacement with matched blood. A serum β-hCG level can confirm pregnancy, but it is less reliable in identifying HP, as levels might be within the normal range owing to the coexisting IUP.13 Monitoring doubling rates might have limited usefulness, as up to 17% of ectopic pregnancies have normal doubling rates.14 Low progesterone levels cannot distinguish between nonviable intrauterine and ectopic pregnancies, and high levels cannot definitively rule out the presence of an additional ectopic pregnancy.15
Emergency department echocardiography is targeted ultrasonography performed by physicians certified by the Canadian Emergency Ultrasound Society.16 For patients who present with abdominal pain and positive β-hCG levels, emergency department echocardiography can be performed to help confirm the presence of an IUP, which thus lowers the probability of ectopic pregnancy. The presence of free fluid on ultrasonography with an IUP should also increase clinical suspicion of HP.16
Pelvic and transvaginal ultrasound is useful but might not provide a definitive diagnosis. A study in 2011 showed that in up to 33% of cases, sonographic reports of a normal IUP gave false reassurance.9 In fact, a 2007 study showed that definitive diagnosis was made by laparoscopy or laparotomy in 74% of cases.2 High clinical suspicion for HP is required, and targeted investigations should be performed to rule out nonobstetric causes of abdominal pain.
Case resolution
The Obstetrics and Gynecology Department is consulted and a right distal salpingectomy is performed without complications. The patient is discharged 2 days later with a viable IUP on ultrasonography.
Conclusion
Early diagnosis of HP is essential to reducing the risk of maternal morbidity and mortality, yet it is often a diagnostic challenge.2 Care should be taken to identify risk factors such as ART, PID, and previous abdominal surgeries. A high degree of clinical suspicion should be maintained, even if bedside or radiology ultrasound findings are normal.
Surgical management is the standard treatment, but nonsurgical approaches are becoming more common. Nonsurgical approaches include methotrexate for patients not wishing to preserve their IUP, as well as potassium chloride ectopic injection.2,17 Intrauterine pregnancy survival rates are promising, with a 2007 article citing a survival rate of 69%.2
Notes
EDITOR’S KEY POINTS
Heterotopic pregnancy is a rare but potentially fatal condition. Its early diagnosis is essential to reducing the risk of maternal morbidity and mortality; however, it is often a diagnostic challenge.
Care should be taken to identify risk factors such as use of assisted reproductive techniques and history of pelvic inflammatory disease, ectopic pregnancy, abdominal adhesions, reconstructive tubal surgery, and salpingectomy.
A live intrauterine pregnancy on ultrasonography cannot rule out heterotopic pregnancy.
POINTS DE REPÈRE DU RÉDACTEUR
La grossesse hétérotopique est un problème rare, mais potentiellement mortel. Il est essentiel d’établir un diagnostic précoce afin de réduire le risque de morbidité et de mortalité chez la mère; malheureusement, elle est souvent difficile à diagnostiquer.
Il faut déterminer les facteurs de risque avec soin, tels que les techniques de reproduction assistée et les antécédents de maladie inflammatoire pelvienne, de grossesse ectopique, d’adhérences abdominales, de chirurgie de reconstruction des trompes et de salpingectomie.
Une grossesse intrautérine vivante à l’échographie n’écarte pas la grossesse hétérotopique.
Footnotes
This article has been peer reviewed.
Cet article a fait l’objet d’une révision par des pairs.
Competing interests
None declared
- Copyright© the College of Family Physicians of Canada
References
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.