Psychoactive Medication and Traffic Safety



Abstract
:1. Introduction
2. Methodology
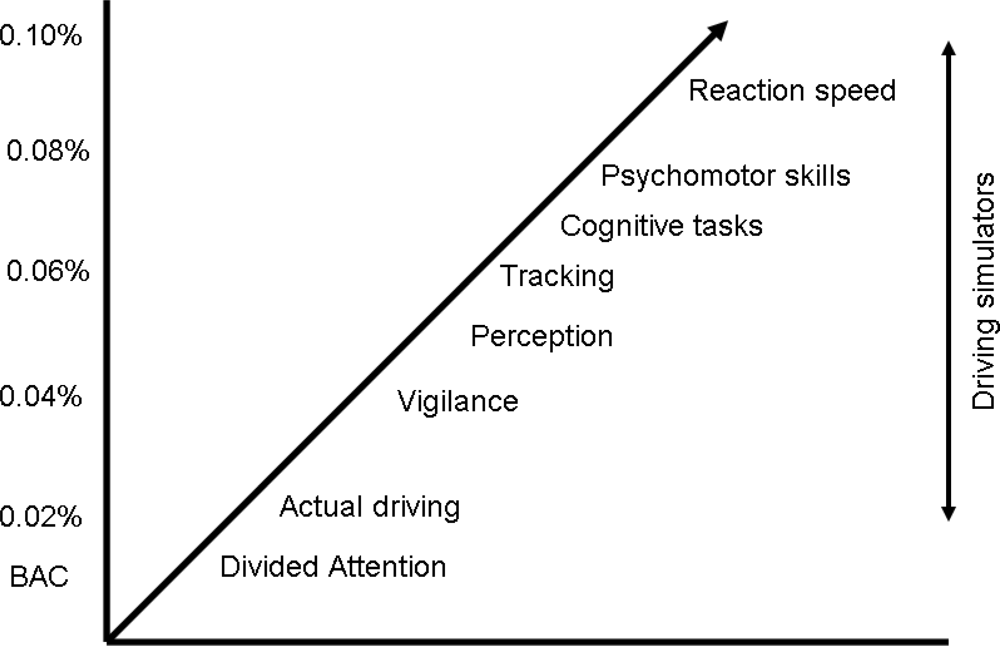
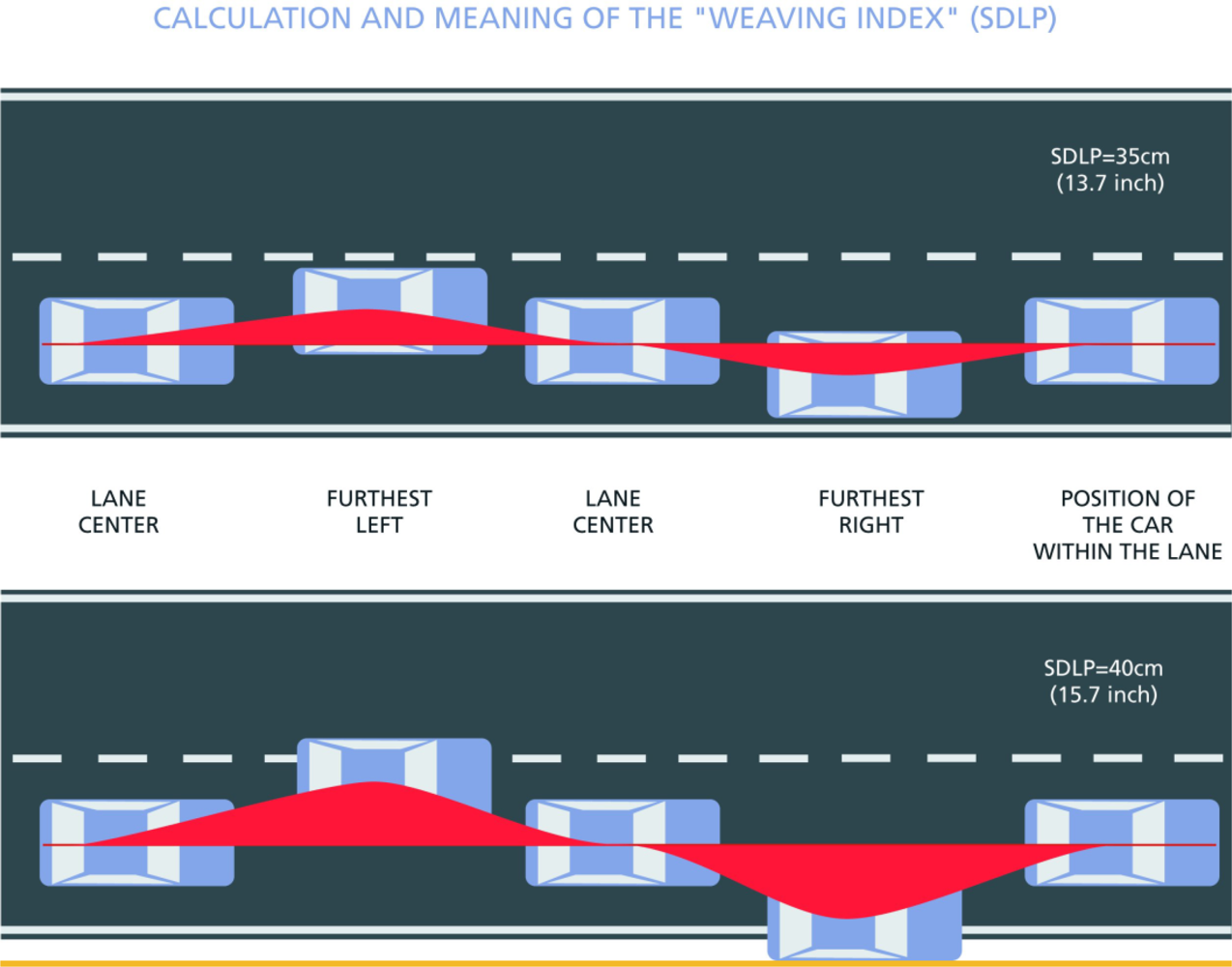
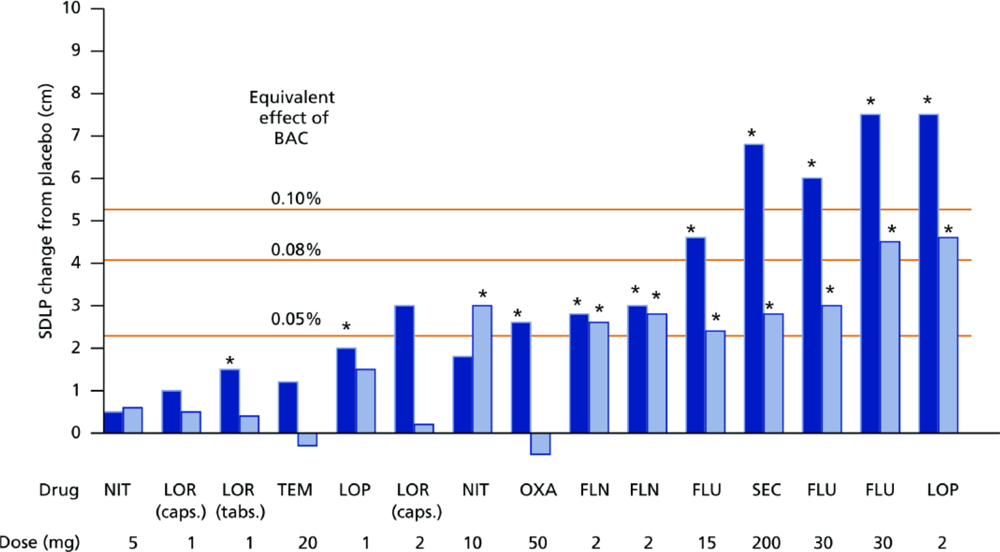
2.1. The On-the-Road Driving Test
2.2. ICADTS Categorization
- Presumed to be safe or unlikely to produce an effect;
- Likely to produce minor or moderate adverse effects;
- Likely to produce severe effects or presumed to be potentially dangerous.
3. CNS Drugs and Traffic Safety
3.1. Hypnotics/Sleep Medication
3.2. Anxiolytics
3.3. Antidepressants
3.4. Antihistamines
3.5. Analgesics
3.6. Stimulant Drugs
4. Conclusions
Disclaimer
References
- Drugs, driving and traffic safety; Verster, JC; Pandi-Perumal, SR; Ramaekers, JHG; De Gier, JJ (Eds.) Birkhauser Verlag: Basel, Switzerland, 2009.
- Global Pharmaceutical Sales 2000–2007. IMS Health Market Prognosis: Norwalk, CT, USA, 2008; http://www.imshealth.com/deployedfiles/imshealth/Global/Content/StaticFile/Top_Line_Data/GlobalSales.pdf (accessed March 28, 2008).
- Peden, M; Scurfield, R; Sleet, D; Mohan, D; Jayder, A; Jarawan, E; Mathers, C. World report on road traffic injury prevention; World Health Organization: Geneva, Switzerland, 2004. [Google Scholar]
- Verster, JC. Measurement of the effects of psychoactive drugs on driving ability and related psychological processes; Ph.D. ThesisUniversity of Utrecht; Utrecht, The Netherlands, October 2002. [Google Scholar]
- Moskowitz, H; Fiorentino, D. A review of the literature on the effects of low doses of alcohol on driving-related skills; US Department of Transportation, National Highway Traffic Safety Administration: Washington, DC, USA; Report DOT HS 809 028, 2000. [Google Scholar]
- Volkerts, ER; van Laar, MW; van Willigenburg, APP. A comparative study of on-the-road and simulated driving performance after nocturnal treatment with lormetazepam 1 mg and oxazepam 50 mg. Hum. Psychopharmacol 1992, 7, 297–309. [Google Scholar]
- O’Hanlon, JF; Haak, TW; Blauw, GJ; Riemersma, JBJ. Diazepam impairs lateral position control in highway driving. Science 1982, 217, 79–81. [Google Scholar]
- Categorization System for Medicinal Drugs Affecting Driving Performance; ICADTS: Oslo, Norway; www.icadts.nl/reports/medicinaldrugs1.pdf (accessed June 26, 2007).
- Louwerens, JW; Gloerich, ABM; De Vries, G. The relationship between drivers’ blood alcohol concentration (BAC) and actual driving performance during high speed travel. In Alcohol, Drugs and Traffic Safety, Proceedings of the 10th International Conference on Alcohol, Drugs and Traffic Safety, Amsterdam, The Netherlands, 9–2 September 1986; Noordzij, PC, Roszbach, R, Eds.; Excerpta Medica: Amsterdam, The Netherlands, 1987; pp. 183–192. [Google Scholar]
- Verster, JC; Veldhuijzen, DS; Volkerts, ER. Residual effects of sleep medication on driving ability. Sleep Med. Rev 2004, 8, 309–325. [Google Scholar]
- Vermeeren, A. Residual effects of hypnotics: epidemiology and clinical implications. CNS Drugs 2004, 18, 297–328. [Google Scholar]
- Verster, JC; Veldhuijzen, DS; Patat, A; Olivier, B; Volkerts, ER. Hypnotics and driving safety: meta-analyses of randomized controlled trials applying the on-the-road driving test. Current Drug Safety 2006, 1, 63–72. [Google Scholar]
- Verster, JC; Volkerts, ER; Schreuder, AHCML; Eijken, EJE; van Heuckelum, JHG; Veldhuijzen, DS; Verbaten, MN; Patat, A; Paty, I. Residual effects of middle-of-the-night administration of zaleplon and zolpidem on driving ability, memory functions, and psychomotor performance. J. Clin. Psychopharmacol 2002, 22, 576–583. [Google Scholar]
- Verster, JC; Volkerts, ER; Johnson, W; Liddicoat, L. Zoplidem and traffic safety – the importance of treatment compliance. Cur. Drug Saf 2007, 2, 220–226. [Google Scholar]
- Barbone, F; McMahon, AD; Davey, PG; Morris, AD; Reid, IC; McDevitt, DG; MacDonald, TM. Association of road traffic accidents with benzodiazepine use. The Lancet 1998, 352, 1331–1336. [Google Scholar]
- Verster, JC; Veldhuijzen, DS; Volkerts, ER. Is it safe to drive a car when treated with anxiolytics? Evidence from on-the-road driving studies during normal traffic. Cur. Psychiat. Rev 2005, 1, 215–225. [Google Scholar]
- Ramaekers, JG. Antidepressants and driver impairment: empirical evidence from a standard on-the-road test. J. Clin. Psychiat 2003, 64, 20–29. [Google Scholar]
- Verster, JC; Volkerts, ER. Antihistamines and driving ability: Evidence from on-the-road driving studies during normal traffic. Annals Allergy, Asthma Immunol 2004, 92, 294–303. [Google Scholar]
- Veldhuijzen, DS; van Wijck, AJM; Verster, JC; Kenemans, JL; Kalkman, CJ; Olivier, B; Volkerts, ER. Acute and subchronic effects of amitriptyline 25 mg on actual driving in chronic neuropathic pain patients. J. Psychopharmacol 2006, 20, 782–788. [Google Scholar]
- Verster, JC; Veldhuijzen, DS; Volkerts, ER. Effects of an opioid (oxycodone/paracetamol) and an NSAID (bromfenac) on driving ability, memory functioning, psychomotor performance, pupil size and mood. Clin. J. Pain 2006, 22, 499–504. [Google Scholar]
- Zacny, JP. Should people taking opioids for medical reasons be allowed to work and drive? Addiction 1996, 91, 1581–1584. [Google Scholar]
- Veldhuijzen, DS; van Wijck, AJM; Wille, F; Verster, JC; Kenemans, JL; Kalkman, CJ; Olivier, B; Volkerts, ER. Effects of chronic nonmalignant pain on highway driving performance. Pain 2006, 122, 28–35. [Google Scholar]
- Ramaekers, JG; Kuypers, KPC; Samyn, N. Stimulant effects of 3-4-methylendioxymethamphetamine (MDMA) 75 mg and methylphenidate 20 mg on actual driving during intoxication and withdrawal. Addiction 2006, 101, 1614–1621. [Google Scholar]
- Verster, JC; Bekker, EM; de Roos, M; Minova, A; Eijken, EJE; Kooij, JJS; Buitelaar, JK; Kenemans, JL; Verbaten, MN; Olivier, B; Volkerts, ER. Methylphenidate and driving ability of adults with attention-deficit hyperactivity disorder: a randomized crossover trial. J. Psychopharmacol 2008, 22, 230–239. [Google Scholar]
- Neutel, I. Benzodiazepine-related traffic accidents in young and elderly drivers. Human Psychopharm. Clin 1998, 13, S115–S123. [Google Scholar]
- Van Laar, MW; Volkerts, ER; van Willigenburg, APP. Therapeutic effects and effects on actual driving performance of chronically administered buspirone and diazepam in anxious outpatients. J. Clin. Psychopharmacol 1992, 12, 86–95. [Google Scholar]
- McGwin, G; Sims, RV; Pulley, L; Roseman, JM. Relationship among chronic medical conditions, medications, and automobile crashes in the elderly: a population-based casecontrol study. Am. J. Epidemiol 2000, 152, 424–431. [Google Scholar]
- Vermeeren, A; Ramaekers, JG; O’Hanlon, JF. Effects of emedastine and cetirizine, alone and with alcohol, on actual driving of males and females. J. Psychopharmacol 2002, 16, 57–64. [Google Scholar]
- Verster, JC; Volkerts, ER; Spence, W; Alford, C; Pandi-Perumal, SR. Hypnotics and daytime functioning: effects of sleep medications on cognition, psychomotor skills, and memory functioning in geriatric patients. Current Psychiat. Rev 2007, 3, 281–292. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Substance name | Category |
|---|---|
| Barbiturates | |
| Secobarbital | III |
| Benzodiazepine derivatives | |
| Flurazepam | III |
| Nitrazepam | III |
| Flunitrazepam | III |
| Estazolam | III |
| Triazolam | III |
| Lormetazepam | III |
| Temazepam | III |
| Midazolam | III |
| Brotizolam | III |
| Quazepam | III |
| Loprazolam | III |
Benzodiazepine related drugs | |
| Zopiclon | III |
| Zolpidem | II |
| Substance name | Category |
|---|---|
| Benzodiazepine derivatives | |
| Diazepam | III |
| Chlordiazepoxide | III |
| Medazepam | II |
| Oxazepam | III |
| Lorazepam | III |
| Bromazepam | III |
| Clobazam | II |
| Ketazolam | III |
| Alprazolam | III |
Azaspirodecandione derivatives | |
| Buspirone | I |
| Substance name | Category |
|---|---|
| Non-selective monoamine reuptake inhibitors | |
| Desipramine | II |
| Imipramine | II |
| Clomipramine | II |
| Amitriptyline | III |
| Nortriptyline | II |
| Doxepin | III |
Selective serotonin reuptake inhibitors | |
| Fluoxetine | I |
| Citalopram | II |
| Paroxetine | I |
| Sertraline | II |
| Fluvoxamine | II |
| Escitalopram | II |
Monoamine oxidase A inhibitors | |
| Moclobemide | II |
Other antidepressants | |
| Mianserin | III |
| Trazodone | III |
| Nefazodone | II |
| Mirtazapine | III |
| Venlafaxine | I |
| Reboxetine | I |
| Substance name | Category |
|---|---|
| Aminoalkyl ethers | |
| Diphenhydramine | III |
| Clemastine | III |
Substituted alkylamines | |
| Dexchlorpheniramine | II |
| Chlorphenamine | II |
| Pheniramine | II |
Phenothiazine derivatives | |
| Promethazine | III |
| Mequitazine | II |
Piperazine derivatives | |
| Meclozine | II |
| Cetirizine | II |
| Levocetirizine | I |
Other antihistamines for systemic use | |
| Triprolidine | III |
| Terfenadine | I |
| Loratadine | I |
| Azelastine | I |
| Ebastine | I |
| Mizolastine | II |
| Fexofenadine | I |
| Desloratadine | I |
© 2009 by the authors; licensee Molecular Diversity Preservation International, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Verster, J.C.; Mets, M.A.J. Psychoactive Medication and Traffic Safety. Int. J. Environ. Res. Public Health 2009, 6, 1041-1054. https://doi.org/10.3390/ijerph6031041
Verster JC, Mets MAJ. Psychoactive Medication and Traffic Safety. International Journal of Environmental Research and Public Health. 2009; 6(3):1041-1054. https://doi.org/10.3390/ijerph6031041
Chicago/Turabian StyleVerster, Joris C., and Monique A.J. Mets. 2009. "Psychoactive Medication and Traffic Safety" International Journal of Environmental Research and Public Health 6, no. 3: 1041-1054. https://doi.org/10.3390/ijerph6031041