Article Text

Abstract
Background: Osteoporotic hip fractures have been extensively studied in women, but they have been relatively ignored in men.
Objective: To study the mortality, morbidity, and impact on health related quality of life of male hip fractures.
Methods: 100 consecutive men aged 50 years and over, with incident low trauma hip fracture, admitted to Royal Cornwall Hospital, UK during 1995–97, were studied. 100 controls were recruited from a nearby general practice. Mortality and morbidity, including health status assessed using the SF-36, were evaluated over a 2 year follow up period.
Results: Survival after 2 years was 37% in fracture cases compared with 88% in controls (log rank test 62.6, df = 1, p = 0.0001). In the first year 45 patients died but only one control. By 2 years 58 patients but only 8 controls had died. Patients with hip fracture died from various causes, the most common being bronchopneumonia (21 cases), heart failure (9 cases), and ischaemic heart disease (8 cases). Factors associated with increased mortality after hip fracture included older age, residence before fracture in a nursing or residential home, presence of comorbid diseases, and poor functional activity before fracture. Patients with fracture were often disabled with poor quality of life. By 24 months 7 patients could not walk, 12 required residential accommodation, and the mean SF-36 physical summary score was 1.7SD below the normal standards.
Conclusions: Low trauma hip fracture in men is associated with a significant increase in mortality and morbidity. Impaired function before fracture is a key determinant of mortality after fracture.
- disease outcomes
- hip fracture
- men
- mortality
- osteoporosis
Statistics from Altmetric.com
Hip fracture is the major adverse clinical and public health consequence associated with osteoporosis. As populations are aging the incidence of hip fractures is increasing.1 The lifetime risk for sustaining hip fracture is estimated at 18% in women and 6% in men.2 Most research on risk factors and outcomes in hip fracture have been undertaken in women. Substantially less information is available for men, although a large number of factors have been suggested to influence male osteoporosis and hip fracture.3,4
In this study we aimed at characterising mortality, morbidity, and impairment in health related quality of life of men with low trauma hip fracture. We also looked at various predictors of mortality, including functional status and levels of residential care. We studied a consecutive series of men with hip fracture who were followed up prospectively for 2 years.
PATIENTS AND METHODS
Study design
A prospective case-control study of male hip fractures was undertaken at the Royal Cornwall Hospital, the only referral centre for orthopaedic trauma in Cornwall. It had no upper age limit, patients and controls came from a well defined geographical area with a homogeneous, stable population, and one single observer made all the clinical observations. Subjects were recruited over a 14 month period to avoid seasonal bias. No subjects dropped out after consent and 100% of survivors were followed up. The study was approved by the local research ethics committee and informed written consent obtained.
Patients
Over 14 consecutive months (in 1995–97), 100 men aged ⩾50 years admitted consecutively to the Royal Cornwall Hospital with a low trauma hip fracture were studied. “Low trauma” was defined as falls from standing height or less. Patients with hip fractures after major trauma, patients not resident in Cornwall, and patients with active malignancy were excluded. Fracture cases were identified by daily review of inpatient admissions to the orthopaedic wards and medical admissions unit: 51 fractures involved the right hip, 48 the left with one bilateral; 55 affected the femoral neck, and 45 were intertrochanteric.
Controls
Simultaneously, “controls” were recruited from a local general practitioner register, comprising men aged ⩾50 years with no history of hip fracture. Subjects with other fractures were not excluded. When a “patient” was identified, an age matched control subject was invited in parallel to participate from a list of 2088 eligible men. If they refused, the next nearest age matched person was invited until a consenting participant was recruited; 185 people were approached to recruit 100 controls. The overall response rate (54%) fell with age (100% for those aged 50–60 years; 50% for those aged over 70 years); reduced response rate from elderly controls made age matching incomplete.
Study protocol
General assessment
Details were recorded of age, residence (own home, other’s home, residential home, nursing home), comorbid conditions (dementia, Parkinson’s disease, heart disease, arthritis, diabetes mellitus, stroke, gastrointestinal disorders), and functional ability measured using the Mediterranean Osteoporosis (MEDOS) Study questionnaire,5 which identifies risk factors 4 weeks before assessment.
Physical examination
Initial standardised clinical assessments of cases and controls included history and examination. Height and weight were recorded in 97 controls and 74 and 85 fracture cases, respectively, with missing observations due to frailty and comorbidities.
Risk factor questionnaires
Interviewer assisted questionnaires at entry collected personal details, mental score, concomitant diseases, drugs, and (for cases) details of the fracture and surrounding circumstances.
Health related quality of life
Health related quality of life was measured with the Short Form-36 (SF-36). Ill health, hearing, visual impairments, poor mental status, and comorbidities made it impossible to collect all data; missing data were obtained where possible from the next of kin or carer.
Bone mineral density (BMD) measurement
Bone mineral density was measured at the lumbar spine and proximal femur by dual energy x ray absorptiometry using Hologic QDR 1000 in cases within 1 week of fracture and in controls at their first visit.6
Follow up
Survivors were reviewed at 6, 12, and 24 months, recording the eight point functional ability questionnaire and SF-36. Vital status and information about current residence was assessed by direct contact with the patient, relative, or carer at 12 and 24 months. Cause of death was obtained from death certificates and postmortem reports.
Statistical analysis
General
Data were analysed using SPSS version 7.5.1 and STATA version 4.0. Descriptive statistics described the frequency of adverse health factors in those with and without hip fracture. For categorical variables, percentages were calculated and significance estimated using Pearson χ2 tests. Odds ratios with 95% confidence intervals were calculated using STATA.
Adjustments
A reduced response rate in elderly controls compromised age matching and consequently all comparisons were age adjusted; additional adjustments were made for other variables, where applicable: BMD was adjusted for age, height, and weight; mortality was adjusted for age and body mass index (BMI).
Mortality
Survival was assessed using Kaplan-Meier curves. A Cox proportional hazards model was used to determine factors linked with increased mortality. To explore the impact on mortality of the comorbid factors we derived a new variable comprising the number of new factors affected.
RESULTS
Subjects were followed up for a mean of 661 days (1.8 years) (range 2–1128 days). Follow up was 100% in both groups. Overall, after 24 months follow up, 58 of the patients with fracture had died, 12 were in institutional care (8 in hospital/nursing home and 4 in residential homes) and 30 were in their own homes. By contrast, eight of the controls had died, 4 were in institutional care (2 in hospital/nursing home and 2 in residential care), and 88 were in their own homes.
Social circumstances
Immediately before admission 71 of the patients with fracture were living in their own or in another’s home, 14 were in a residential home, and 15 in a nursing home (table 1⇓).
Baseline characteristics of cases and controls
General health
Patients with fracture weighed less (mean (SD) 67.8 (11.2) kg) than controls (77.7 (16.3) kg) and had a lower mean BMI (cases 23.4 (3.3) kg/m3; controls 26.7 (5.5) kg/m3). There was no difference in height. Mini-mental score examination differed in cases (within 48 hours of fracture) and controls (at first visit); 48 cases and 84 controls scored 10; 15 cases and 3 controls scored ⩽5. Mental status could not be assessed in nine cases with dementia.
Comorbid conditions
Comorbidities were identified in 79 cases and 54 controls (χ2 = 13.8; df = 1, p<0.001); 47 cases had two or more comorbid conditions compared with 18 controls (χ2 = 29.7, df = 7, p<0.0001) (table 1⇑). Poor vision, Parkinson’s disease, dementia, reduced mobility, and a history of falls were more commen in cases. No patients were receiving oral steroids in the 12 months before their fracture; there were no differences between cases and controls in the frequency of intake of any drugs that might be linked to developing osteoporosis.
Bone mineral density
Cases had significantly lower BMD at all sites than controls. T scores <−2.5 at the femoral neck were present in 48/58 (83%) fracture cases who had a scan compared with 39/100 (39%) controls. After adjusting for age, height, and weight, the risk of hip fracture was substantial per 0.1 mg/cm2 decrease in bone mass: for the lumbar spine odds ratio (OR) = 1.2 (95% confidence interval (CI) 1.0 to 1.6); for the femoral neck OR = 2.0 (95% CI 1.3 to 3.1). These BMD findings have been reported previously.6
Morbidity
Residential status
Twelve months after fracture 55 patients were still alive; 35 were at home, and 20 in residential accommodation (6 in residential homes; 14 in nursing homes). All 35 patients at home 12 months after fracture had been living at home before fracture; 8 patients who had been at home before fracture were in residential care. The situation was similar 24 months after fracture, with 30 of the 42 surviving cases still at home. Most controls (93 and 88, respectively) continued to live in their own homes at 12 and 24 months.
Functional status
Health Assessment Questionnaire (HAQ) scores were available for 91, 50, 47, and 35 patients and for 99, 97, 87, and 84 controls at baseline, 6, 12, and 24 months, respectively. The mean HAQ score in the hip fracture cases was 0.84 at baseline, and this rose to 1.2 in the 50 survivors at 6 months and stabilised at 1.2 in the fracture survivors at 12 and 24 months. In controls the mean HAQ score at first visit was 0.27 and increased slightly to 0.39 at 24 months (fig 1⇓).

Change in health using the Health Assessment Questionnaire (HAQ) over 24 months.
Mobility
Details of mobility 12 months after fracture were available in 47 cases: 17 (36%) could walk independently; 7 (15%) could not walk. Data from 87 controls showed that 73 (84%) walked normally and only 1 (1%) could not walk. Details at 24 months after fracture were available from 35 cases: 12 (34%) could walk independently; 7 (20%) could not walk. Data from 84 controls showed 71 (85%) walked normally; none were unable to walk.
Health related quality of life
Eighty one patients completed the SF-36 questionnaire within 48 hours of their fracture. Follow up scores at 6, 12, and 24 months were available for 51, 47, and 34 cases respectively. All controls completed the SF-36 questionnaire at baseline and 97, 87, and 84 controls at 6, 12, and 24 months, respectively. Baseline SF-36 scores in the cases, reflecting health status before fracture, were significantly worse than in controls for all domains except pain.
Composite physical and mental component scores showed that cases before fracture had worse overall health than controls. Mean physical scores before fracture in cases were more than 1SD below the standard US means. Mental scores before fracture, although less than in controls, were not abnormal by US standards. The immediate effect of fracture was seen on the physical but not on the mental component summary scores; after fracture, physical scores deteriorated steadily to more than 1.7SD below the US mean at 2 years. The fracture did not have an immediate effect on the mental scores, though 2 years after fracture there had been a significant decline in mental component scores (p<0.04).
Mortality
Fifty eight patients with hip fracture died; early mortality (at 90 days) was 25%. More deaths occurred in the first (45) than the second year (13). Twelve survivors at 2 years were in care and 30 in their own home. At 2 years only 8 controls had died, 4 were in hospital, nursing home, or residential home and 88 were in their own home. The Kaplan-Meier survival curves (fig 2⇓) illustrate the excess of deaths in fracture cases compared with controls. This difference was most marked in the first 3 months after fracture. Overall survival among the cases was 37% compared with 88% in controls (log rank test 62.6, df = 1, p = 0.0001). In the first year of observation 45 patients died but only one of the controls. By the end of follow up 60 patients but only 10 controls had died. Patients with hip fracture died from various causes (table 2⇓), including bronchopneumonia (21 cases), heart failure (9 cases), and ischaemic heart disease (8 cases). There was no evidence that bronchopneumonia or heart failure occurred at different times after fracture. Of 21 deaths due to bronchopneumonia, six occurred by 1 month, nine between 1 and 6 months, and six after 6 months.
Causes of death among cases and controls

Kaplan-Meier survival curves among cases and controls. Overall survival among the cases was 37% compared with 88% in controls (log rank test 62.6, df = 1, p = 0.0001).
Age greatly influenced mortality (log rank 24.8, df = 1, p = 0.0001). Survival was 100% when the hip fracture occurred in the 5th decade, only 50% in the 7th decade, and all but one patient aged > 90 years died.
Predictors of mortality
Overall predictors
Cox regression analysis (table 3⇓) confirmed that mortality was significantly higher in hip fracture cases than in controls (hazards ratio (HR) = 9.3 (95% CI 4.8 to 16.3); p<0.0001). This excess mortality persisted after adjusting for age (HR (95% CI) 8.1 (4.1 to 16.0)) and body mass index (HR (95% CI) 7.8 (3.6 to 16.9)) After controlling for quality of life before fracture using the physical component domain of the SF-36 or HAQ scores, fracture cases continued to show a six- to sevenfold excess mortality compared with controls (HR = 6.2–7.2). There were insufficient deaths by specific causes to examine reliably whether differences in status before fracture predicted specific types of death.
Influence of hip fracture on mortality: cases versus controls
Residence, comorbidity, and physical function
After adjusting for age using Cox regression analysis only institutional care at the time of hip fracture, the presence of a comorbidity, and poor physical function before fracture were significant predictors of mortality (table 4⇓). The presence of one or more comorbid diseases at the time of fracture more than doubled the risk of dying (HR = 2.8). Mortality exceeded 70% when another disease was present but was <40% in the absence of a concomitant disease.
Influence of baseline characteristics on mortality after hip fracture
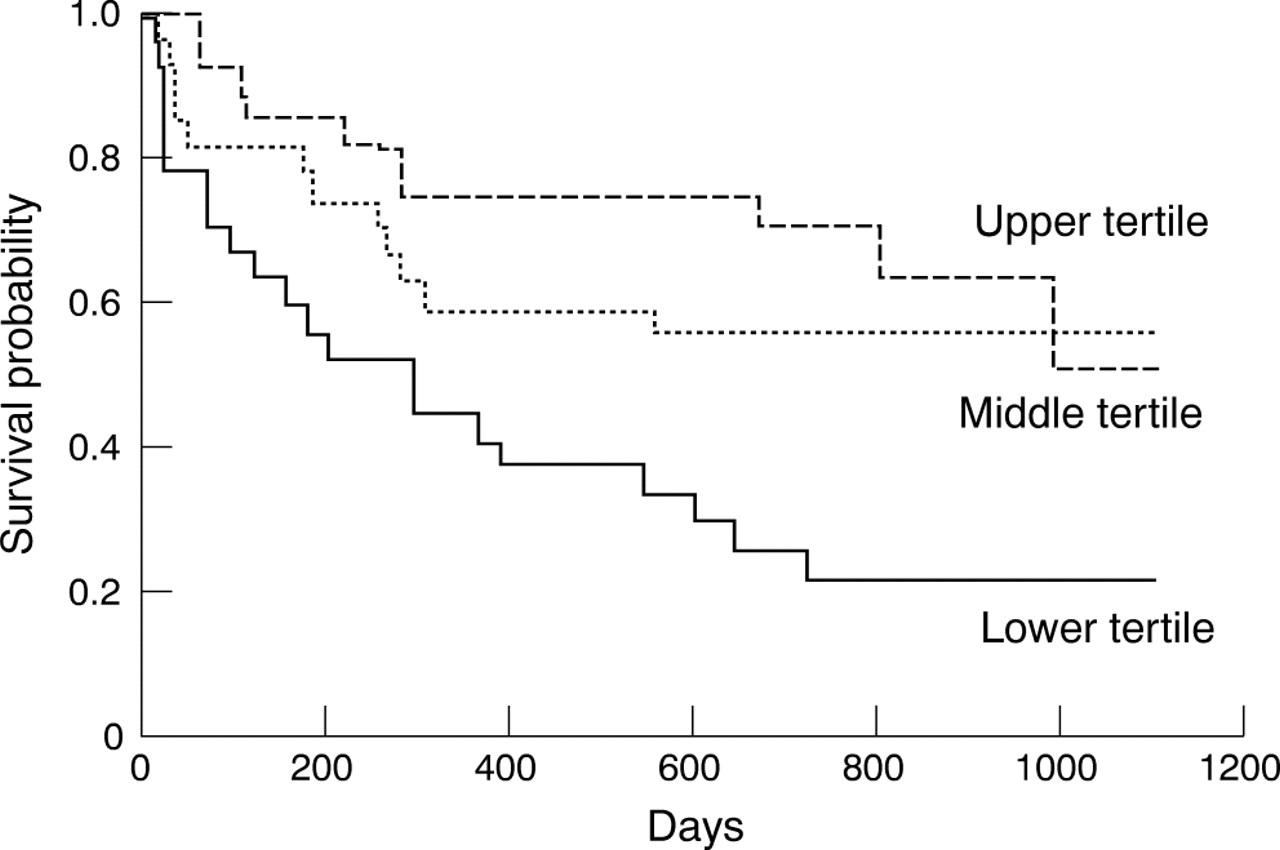
The initial physical component score from the SF-36, available in 81 cases, was a highly significant predictor of mortality (log rank test 11.6, df = 2, p = 0.003): 21 (78%) cases in the lowest tertile had died by 2 years compared with 12 (44%) in the middle and 10 (37%) in the highest tertiles. Patients in the lowest tertile for physical component scores had high immediate mortality after fracture; only 21 (78%) surviving for 1 month and 6 (22%) for 2 years. No patients in the highest tertile died in the first 2 months after fracture; their 2 year survival was 70% (fig 3⇓).
{kind=link}
{kind=link}
{kind=link}
Kaplan-Meier survival curves for cases stratified by initial physical component score of the SF-36.
Stepwise multiple regression with age, functional capacity, and residence in the equation showed that age and functional capacity were good predictors of excess mortality, with hazards ratios of 1.1 and 1.5, respectively. After adding comorbidity to the regression equation, the only significant variable influencing mortality was age. On substituting a cut off point of 70 years for age into the regression equation, the significance of age on mortality was more apparent (HR = 4.6, 95% CI 1.4 to 15.0; p<0.01). In this analysis baseline functional capacity no longer retained significance (HR = 1.3, 95% CI 0.9 to 1.8, p = NS). Repeat analysis replacing functional capacity (HAQ) with the physical component score did not alter the results. Age and baseline physical component score were the only variables that significantly influenced mortality; age was dominant.
DISCUSSION
We found a six- to sevenfold increased risk of death in male hip fracture cases compared with population controls. Such excess mortality,7 which is particularly high in men,8 has been well described. Thirty four observational studies have reported mortality data in male hip fractures9–,42; with few exceptions,12,25 most found that men had higher mortalities, including evaluations of mortality compared with age and sex matched controls10 and deaths in the general population.12 Mortality rates varied from 11%9 to 71%,20 with in-hospital mortality between 2%12 and 37%.15 Such differences reflect variations in case selection and characteristics of the populations studied. The risk of death is greatest immediately after the fracture and decreases over time,7 with few deaths directly attributed to the hip fracture and most reflecting the chronic illnesses predisposing towards fracture.
Our data reflect these views: 45/60 deaths in our cases occurred during the first year after fracture; 38 were caused by pneumonia and heart disease. Although male hip fracture is a pre-terminal event in some cases, there is good evidence that it also shortens life; Trombetti and colleagues calculated that after hip fracture male life expectancy is reduced by an average of 5.8 years.32 We found no deaths due to pulmonary thromboembolic disease; the local hospital policy, which used heparin to anticoagulate hip fracture cases, appears effective.
Most fracture survivors in our study had reduced function, poor quality of life, and increased dependency. An important impairment was inability to walk: 12 months after fracture only 17/47 (36%) of our patients walked independently; and at 24 months only 12/35 (34%) patients. We assessed function with the MEDOS questionnaire; we do not believe using a form developed in southern Europe was inappropriate in Cornwall. Our findings are slightly worse than walking ability after fracture reported in mixed sex series. For example, one early retrospective analysis of 360 patients with hip fractures reported that 22% were non-ambulatory 12 months after fracture,43 and a recent retrospective study of 280 patients with hip fractures in Singapore44 found that 28% of those alive at 1 year could walk without aids.
The SF-36 showed that before fracture our cases had significantly worse overall health than controls; mean physical component SF-36 scores were more than 1SD below standard US mean levels. As we could not assess the SF-36 in some of our fracture cases, and these patients had very poor health, excluding them will have enhanced the apparent health status of the fracture group as a whole. After fracture physical scores deteriorated steadily to more than 1.7SD below the US mean levels at 2 years. There was an associated decline in SF-36 mental component scores. Comparable findings with the SF-36 have been reported in several studies of male and female hip fracture cases,45–,47 including the low baseline quality of life scores.48 The need for long term care shows the extent of dependency; in our cases 12 survivors required residential accommodation after 24 months. The high frequency of institutionalisation after fracture has been well described. Diamond and colleagues reported that 50% of men were institutionalised 12 months after fracture,24 though other series of men and women report slightly lower rates of institutionalisation,49 with large differences between centres.50 There is some evidence that management approaches, like care pathways, reduce the number of cases who become institutionalised.51
The strong points of our study include evaluating consecutive men with hip fracture from a single area of the UK, with prospectively collected complete follow up data. One limitation was incomplete response rates for participation in the control group, which reduced with increasing age, making our controls younger than fracture cases. Although adjustments were made when analysing mortality, if potential controls who declined to participate had poorer health, the excess mortality and poor outcomes of fracture cases might have been overestimated. A second limitation was that status before fracture was defined after fracture, when recall might have been impaired, with resultant misclassification. Finally, Cornwall is a rural area and evidence shows that hip fracture rates are lower in rural communities52; our findings may therefore not be completely generalisable.
In conclusion, we have shown that low trauma hip fracture in men results in a significant increase in mortality and morbidity. After 24 months, of 100 fracture cases, 58 were dead, 12 were in institutional care, and only 30 remained in their own homes. Age and impaired function before fracture were key determinants of mortality after fracture.
Acknowledgments
We acknowledge support to the Royal Cornwall Hospital from the UK National Health Service (NHS) Research and Development Programme. We are also grateful to the ARC (http://www.arc.org.uk; accessed 27 September 2005) for supporting research activities in our units.
REFERENCES
Footnotes
Published Online First 3 August 2005
The authors have no conflicts of interests.