Article Text

Abstract
Background Brain tumours are the commonest solid tumour in children. Children with brain tumours are frequently unwell for months prior to diagnosis. A prolonged period between symptom onset and diagnosis is associated with increased morbidity.
Objective To develop an evidence-based clinical guideline to support healthcare professionals in the identification, assessment and investigation of children presenting with symptoms and signs that could be due to a brain tumour.
Methods A systematic literature review with a meta-analysis and cohort study provided the guideline evidence base. A multi-disciplinary workshop and Delphi consensus voting were used to translate the evidence into a clinical guideline. The results of the literature review and cohort study have been previously published.
Results 20 healthcare professionals and parents participated in the workshop. 77 statements were generated detailing the presenting features of childhood brain tumours, factors that could be used to discriminate brain tumours from other less serious conditions and possible referral pathways for children with brain tumours. 156 healthcare professionals agreed to participate in the Delphi process; 112 completed the first round and 88 completed all three rounds (attrition rate 21%). 64 statements reached consensus. The final guideline comprises 76 recommendations advising on the symptomatology of childhood brain tumours, assessment of children who may have a brain tumour and recommendations for selection for and timing of central nervous system imaging.
Conclusion Implementation of this guideline may support clinicians in the identification and timely imaging of children with brain tumours. This may reduce the morbidity currently experienced by many children with brain tumours.
Statistics from Altmetric.com
Introduction
One in 600 children under the age of 16 will be affected by cancer (a similar prevalence to childhood cerebral palsy, diabetes mellitus and meningitis).1,–,3 A quarter of all children with cancer have a central nervous system (CNS) tumour and these tumours are now the commonest cause of death from cancer in childhood.4,–,6 Sixty per cent of children who survive a brain tumour are left with life altering disability.7,–,12
Despite the widespread availability of CNS imaging, many children with a brain tumour in the UK are unwell for months prior to diagnosis. Two recent UK cohorts of children with brain tumours had median symptom intervals (time between symptom onset and diagnosis) of 2.5 and 3.5 months,13 14 up to three times longer than that experienced by children in North America, Poland, Israel and Switzerland.15,–,19 Children with brain tumours who experience a long symptom interval are more likely than those who are diagnosed rapidly to present with life threatening complications, have frequently developed irreversible neurological deficits by diagnosis (particularly visual loss and endocrinopathies) and show greater cognitive deficits in later life.20,–,25 A prolonged time to diagnosis undermines the trust patients and their families have in the UK healthcare system and often leads to significant psychological distress.26
What is already known about this topic
▶. The initial presentation of brain tumours in children frequently mimics other more common and less serious conditions, resulting in diagnostic difficulty and a prolonged time to diagnosis (symptom interval).
▶. A prolonged symptom interval is associated with increased morbidity, increased cognitive impairment and significant psychological distress.
What this study adds
▶. The Children's Brain Tumour Research Centre at Nottingham University has developed an evidence-based guideline to support clinicians in the identification, assessment and investigation of children who may have a brain tumour.
Current referral guidelines for suspected cancer (including specific guidance for children and young people) were developed by The UK National Collaborating Centre for Primary Care and were issued by the National Institute for Health and Clinical Excellence (NICE) in June 2005.27 While this provides a concise summary of the common modes of brain tumour presentation in children, it has three important limitations. First, it is predominantly directed at primary care, whereas diagnostic difficulties for children with brain tumours occur throughout the health service. Second, the ‘end point’ for the NICE guidelines is referral. Brain tumours are diagnosed by imaging rather than referral and so guidance is required on indications for, and appropriate waiting times to, imaging. Finally, the guidance is based on a limited evidence base (13 references published between 1978 and 2002).
Many families of children affected by a brain tumour believe that a diagnosis was only reached following repeated insistence on their part that their child was unwell, and that in the absence of this the diagnosis would have been (even more) delayed.26 This perception, combined with the published evidence suggesting that UK children with a brain tumour experience a longer symptom interval than children in many other countries, resulted in the Pathways Project, a collaboration between healthcare professionals and service users established to provide improved guidance for healthcare professionals on the assessment, investigation and referral of children who present with symptoms and signs that could result from a brain tumour.
We have previously reported a systematic review and meta-analysis of the literature on childhood brain tumour presentation published between 1991 and 200528 and a cohort study of children newly diagnosed with a brain tumour at four UK paediatric neuro-oncology centres between 2004 and 2006.14 These reports provided information on the signs and symptoms that occur in children with brain tumours, their progression and factors associated with a prolonged symptom interval. However, they do not address the question of the likelihood of a child with a given symptom or sign having a brain tumour, that is, its specificity, and there are no previous studies addressing this, except in the case of seizures29 and to an extent, headaches.30 The questions of specificity, referral pathways, imaging indications and acceptable waiting times cannot easily be addressed by quantitative research methods. Qualitative methods in the form of a multi-disciplinary workshop and a Delphi consensus process31 were therefore used to incorporate the evidence from the meta-analysis and cohort study into a clinical guideline.
Methods (figure 1)
Multidisciplinary workshop
Twenty healthcare professionals and parents of children with brain tumours attended the workshop (see online document for workshop participants). The workshop reviewed the data obtained from the meta-analysis and cohort study and examined symptoms, signs and management decisions identified by literature review and data collection as being key to the diagnosis. Workshop participants worked in small groups and were asked to devise statements on the following for each of the key areas: symptoms and signs, factors influencing specificity, clinical assessment, thresholds for referral and selection for imaging, and best practice for referral and imaging. The workshop participants discussed the conclusions from each group and devised a series of statements for subsequent consideration by a Delphi panel.

The Delphi process.
Delphi process
Letters of invitation to join the Delphi panel were sent to health specialists involved in the prediagnostic care of one or more of the 144 patients recruited to the cohort study or with membership of a professional body involved in the care of children with brain tumours. (See online document for Delphi panel composition, details of the Delphi process and discussion of its role in guideline development.)
Ethics
Approval was granted by Nottingham 2 REC.
Results
The workshop participants and research team devised 77 statements describing the presenting features of childhood brain tumours, factors that could be used to discriminate brain tumours from other less serious conditions and possible referral pathways for children with brain tumours. These statements were peer reviewed via three rounds of a Delphi process. A total of 156 healthcare professionals agreed to participate in the Delphi process; 112 completed the first round and 88 completed all three rounds (attrition rate 21%).
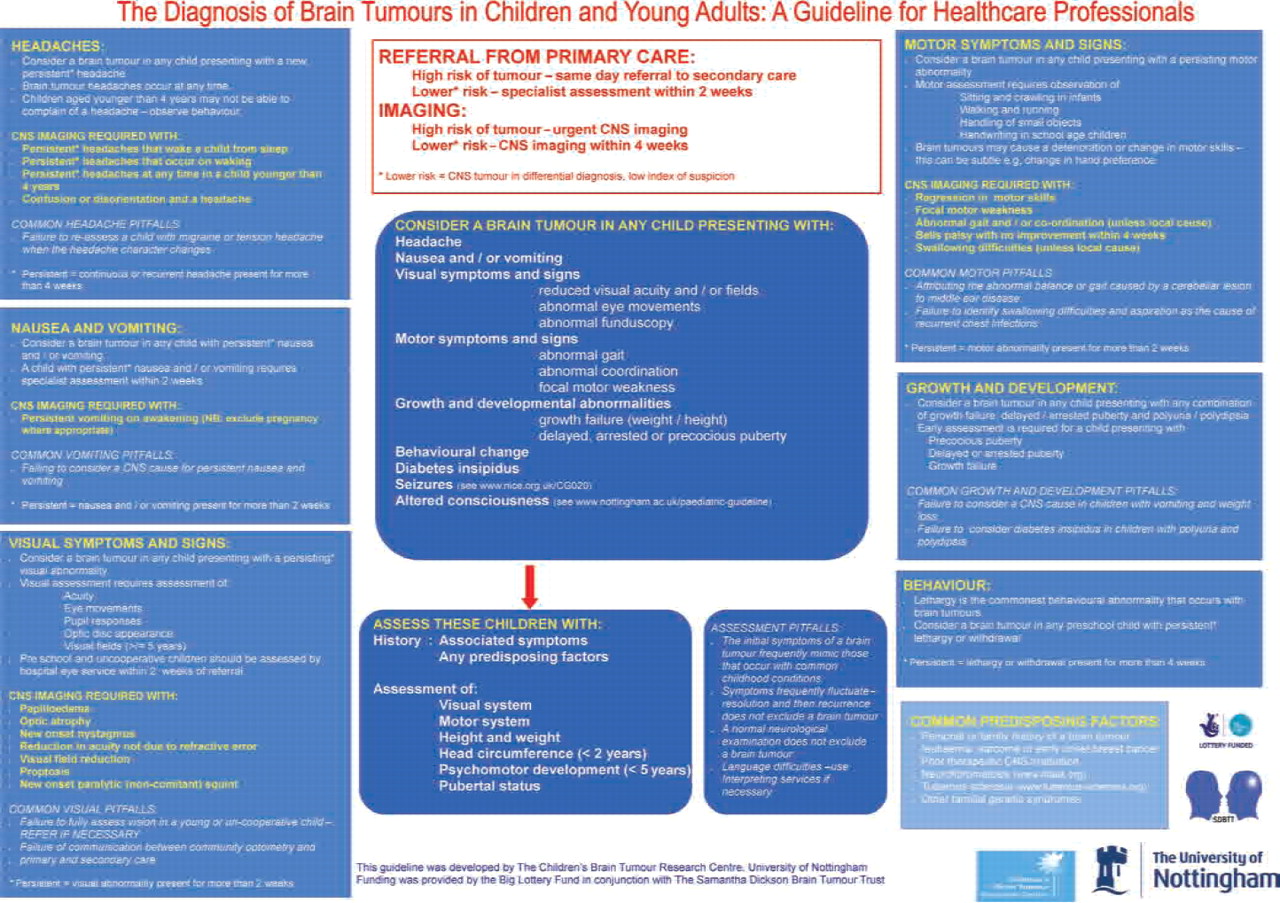
The final guideline is shown below. There are 76 recommendations. The levels of evidence, recommendation grades (according to SIGN (Scottish Intercollegiate Guidelines Network) 2000)32 and, where appropriate, degree of consensus for each statement are reported in the online version. A one-page quick reference summary is shown in figure 2. The complete guideline including supporting evidence and Delphi questionnaires can be viewed at http://www.rcpch.ac.uk/Research/CE/Guidelines-frontpage/Guideline-Appraisals-by-Topic/RCPCH-Summary-and-Appraisals-Cancer#CANCER.

{kind=link}
{kind=link}
Guideline summary.
Best practice
Consultation
▶. Parents and their carers should be asked explicitly about their concerns in any consultation.
▶. If a parent/carer expresses concerns about a brain tumour, this should be reviewed carefully. If a brain tumour is unlikely, the reasons why should be explained and arrangements made for review within 4 weeks.
▶. If the patient, parent/carer and healthcare professional are not fluent in a common language, an interpreter must be used for the consultation (http://www.languageline.co.uk).
▶. Low parental educational level, social deprivation and lack of familiarity with the UK healthcare system may be associated with diagnostic delay. A lower threshold for investigation and referral may be appropriate in these situations.
Referral
▶. A primary healthcare professional who has a high index of suspicion regarding a possible brain tumour should discuss their concerns with a secondary healthcare professional the same day.
▶. A child referred from primary care in which the differential diagnosis includes a possible space occupying lesion should be seen within 2 weeks.
Imaging
▶. A child in whom CNS imaging is required to exclude a brain tumour (potential diagnosis but low index of suspicion) should be imaged within 4 weeks.
▶. MRI is the imaging modality of choice for a child who may have a brain tumour.
▶. If MRI is not available, a contrast enhanced CT should be performed.
▶. Imaging results should be interpreted by a professional with expertise and training in CNS MR and CT imaging in children.
▶. The need to sedate or anaesthetise a child for imaging should not delay imaging by more than 1 week.
Feedback
▶. Patients and their families should receive the provisional results of CNS imaging within 1 week of the investigation.
Predisposing factors
The following are all associated with an increased risk of childhood brain tumours. Their presence may lower the threshold for referral and investigation:
▶. Personal or family history of a brain tumour, leukaemia, sarcoma or early onset breast cancer
▶. Prior therapeutic CNS irradiation
▶. Neurofibromatosis 1 and 2
▶. Tuberous sclerosis 1 and 2
▶. Other familial genetic syndromes
Presentation and assessment of a child with a potential brain tumour
Presenting symptoms and signs
The following symptoms and signs are all associated with childhood brain tumours. Their presence should alert the clinician to this possibility.
▶. Headache
▶. Nausea and/or vomiting
▶. Visual symptoms and signs including
▷. - Reduced visual acuity
▷. - Reduced visual fields
▷. - Abnormal eye movements
▷. - Abnormal funduscopy
▶. Motor symptoms and signs including
▷. - Abnormal gait
▷. - Abnormal co-ordination
▷. - Focal motor abnormalities
▶. Growth and developmental abnormalities including
▷. - Growth failure
▷. - Delayed, arrested or precocious puberty
▶. Behavioural change
▶. Diabetes insipidus
▶. Seizures – not covered in this guideline (see http://www.nice.org.uk/CG020)
▶. Altered consciousness – not covered in this guideline (see http://www.rcpch.ac.uk/Research/CE/Guidelines-frontpage/Guideline-Appraisals-by-Topic/RCPCH-Summary-and-Appraisals-Emergency-Medicine)
Symptoms and signs in childhood brain tumours may occur singularly or in combination.
History
Take a detailed history and enquire specifically about:
▷. - Associated symptoms
▷. - Predisposing factors
Assessment
Assess:
▷. - Visual system
▷. - Motor system
▷. - Height and weight
▷. - Head circumference if under 2 years of age
▷. - Pubertal status
▶. The initial symptoms of a brain tumour frequently mimic those that occur with many common childhood conditions.
▶. Symptoms frequently fluctuate in severity – resolution and then recurrence does not exclude a brain tumour.
▶. Presentation depends upon the age of the child.
▶. A normal neurological examination does not exclude a brain tumour.
Signs and symptoms of a child with a potential brain tumour
Headache:
▶. Consider a brain tumour in any child presenting with a new persistent headache. (A continuous or recurrent headache lasting for more than 4 weeks should be regarded as persistent.)
▶. Brain tumour headaches can occur at any time of the day or night.
▶. Children aged younger than 4 years, or those with communication difficulties, are frequently unable to describe headache; their behaviour, for example, withdrawal and holding their head may indicate a headache.
▶. In a child with a known migraine or tension headache, a change in the nature of the headache requires reassessment and review of the diagnosis.
CNS imaging (within a maximum of 4 weeks) required for:
▶. Persistent headaches that wake a child from sleep
▶. Persistent headaches that occur on waking
▶. A persistent headache occurring at any time in a child younger than 4 years
▶. Confusion or disorientation occurring with a headache
Delayed diagnosis has been associated with:
▶. Failure to reassess a child with migraine or tension headache when the headache character changes
Nausea and vomiting:
▶. Early specialist referral for consideration of underlying causes including CNS causes is required for a child with persistent nausea and/or vomiting. (Nausea and/or vomiting that lasts for more than 2weeks should be regarded as persistent.)
CNS imaging (within a maximum of 4 weeks) required for:
▶. Persistent vomiting on awakening (either in the morning or from a day time sleep). NB: Exclude pregnancy where appropriate.
Delayed diagnosis has been associated with:
▶. Attributing persistent nausea and vomiting to an infective cause in the absence of corroborative findings, eg, contact with similar illness, pyrexia, diarrhoea
Visual symptoms and signs:
▶. Consider a brain tumour in any child presenting with a persisting visual abnormality. (Any visual abnormality lasting longer than 2 weeks should be regarded as persistent.)
Visual assessment must include assessment of:
▷. - Pupil responses
▷. - Acuity
▷. - Visual fields in school age children
▷. - Eye movements
▷. - Optic disc appearance
▶. If the assessing healthcare professional is unable to perform a complete visual assessment, the child should be referred for assessment.
▶. Children referred for visual assessment should be seen within 2 weeks of referral.
▶. Community optometry should refer any child with abnormal eye findings (excluding simple refractive errors) directly to secondary care.
▶. Preschool and uncooperative children should be assessed by the hospital eye service.
▶. A child with a new onset non-paralytic (concomitant) squint should have early ophthalmological assessment for consideration of underlying causes (including CNS causes).
Delayed diagnosis has been associated with:
▶. Failure to fully assess vision in a young or uncooperative child
▶. Failure of communication between community optometry and primary and secondary care
CNS imaging (within a maximum of 4 weeks) required for:
▶. Papilloedema
▶. Optic atrophy
▶. New onset nystagmus
▶. Visual field reduction
▶. Proptosis
▶. New onset paralytic (non-concomitant) squint
Motor symptoms and signs:
▶. Consider a brain tumour in any child presenting with a persisting motor abnormality. (Any motor abnormality lasting longer than 2 weeks should be regarded as persistent.)
▶. Brain tumours may cause a deterioration or change in motor skills; this may be subtle, for example, a change in hand or foot preference, loss of learnt skills (computer games).
Motor system assessment must include observation of:
▷. - Sitting and crawling in infants
▷. - Walking and running
▷. - Coordination, for example, heel to toe walking
▷. - Handling of small objects
▷. - Handwriting in school age children.
CNS imaging (within a maximum of 4 weeks) required for:
▶. A regression in motor skills
▶. Focal motor weakness
▶. Abnormal gait and/or coordination (unless local cause)
▶. Bell's palsy (isolated lower motor facial palsy) with no improvement within 4 weeks
▶. Swallowing difficulties (unless local cause)
Delayed diagnosis has been associated with:
▶. Attributing abnormal balance or gait to middle ear disease in the absence of corroborative findings
▶. Failure to identify swallowing difficulties as the cause of recurrent chest infections or “chestiness”
Growth and development:
Consider a brain tumour in any child presenting with any two of the following:
▷. - Growth failure
▷. - Delayed or arrested puberty
▷. - Polyuria and polydipsia
Early referral (from primary care) is required for a child presenting with:
▷. - Precocious puberty
▷. - Delayed or arrested puberty
▷. - Growth failure
▶. Early specialist referral for consideration of underlying causes including CNS causes is required for a child presenting with precocious puberty.
▶. Diabetes insipidus must be considered in a child presenting with polyuria and/or secondary nocturnal eneuresis.
Delayed diagnosis has been associated with:
▶. Attributing impaired growth with vomiting to gastrointestinal disease in the absence of corroborative findings
▶. Failure to consider diabetes insipidus in children with polyuria and polydipsia
Behaviour:
▶. Lethargy is the commonest behavioural abnormality that occurs with brain tumours.
▶. Environmental context is important when assessing lethargy: a child who is lethargic in situations in which they are normally active requires further assessment.
Discussion
Childhood brain tumours have a heterogeneous presentation dependent upon the tumour location, tumour biology and age of the child.28 This frequently leads to a prolonged symptom interval, which is associated with increased morbidity, increased cognitive impairment and significant psychological distress for the patient, their family and the responsible healthcare professionals.20,–,26 Rapid diagnosis relies on clinicians considering the diagnosis with many different, common presenting symptoms and signs, searching for corroborative evidence and instigating imaging where appropriate. This evidence-based guideline supports this process by listing the presenting symptomatology of childhood brain tumours, advising a structured assessment of children who present with these symptoms and signs and listing indications, with specific time limits, for referral and imaging. Implementation of the guideline aims to increase the knowledge of childhood brain tumours among healthcare professionals, and thus reduce the possibility that a brain tumour is inappropriately excluded from a differential diagnosis.
This specific method of guideline development has several strengths. The guideline is based upon best available evidence; the meta-analysis summarised the presentation of brain tumours and identified the influence of age and tumour location28 and the cohort study provided contemporary information on childhood brain tumour presentation, assessment and diagnosis in UK centres.14 Stakeholder involvement was achieved with a multi-disciplinary workshop involving a broad range of professionals and service users and with a Delphi consensus process.
The guideline adds to the NICE ‘Referral guidelines for suspected cancer in adults and children’27 by extending the guideline scope to secondary as well as primary care, by providing specific advice to clinicians on the assessment and selection of children for imaging, by specifying maximum observation and waiting times for imaging, and by an improved evidence base.
This guideline also has limitations. The guideline is the opinion of the Delphi group, which may include collective error where supportive evidence is lacking. The level of evidence for each recommendation is detailed in both the guideline website and in the online version of this paper, thus enabling clinicians to see which statements have a strong evidence base. The full guideline is long; however it has been structured to help clinicians identify the relevant area rapidly and includes a summary page and potential wall chart (figure 2). The guideline does not refer to evidence published subsequent to the literature review and Delphi process; the development group will review the evidence base and repeat the literature search 5 years after publication and combine it with audit and feedback from guideline users to update the guideline.
We are currently developing a dissemination and education programme to support guideline implementation in conjunction with the Royal Colleges of Paediatrics and Child Health, General Practice and Radiologists, with the College of Emergency Medicine and with the Health Foundation. We believe that guideline implementation will help reduce the prolonged symptom interval and resultant morbidity currently experienced by many children with brain tumours.
Acknowledgments
The authors would like to thank the Delphi workshop participants and Delphi panel members for the time and expertise they gave to the guideline development process.
References
Footnotes
-
Funding The guideline was developed with a grant (grant number RG10044964) from the Big Lottery Fund. The grant was applied for by The Samantha Dickson Brain Tumour Trust (registered charity no.1060627) on behalf of the Children's Brain Tumour Research Centre, University of Nottingham. The funders had no role in study design, data collection, data analysis, data interpretation or writing of this report.
-
Competing interests None.
-
Ethics approval This study was conducted with the approval of the Nottingham 2 REC.
-
Provenance and peer review Not commissioned; externally peer reviewed.