Article Text

Abstract
Background Over the last decade, there has been a significant increase in the number of cutaneous abscesses. While there is general agreement that abscesses should be treated with incision and drainage, it is unclear whether systemic antibiotics should be routinely prescribed.
Objective To evaluate whether systemic antibiotics, when compared with a placebo, improve cure rates in patients with simple abscesses after incision and drainage.
Methods Design Systematic review and meta-analysis using RevMan5.
Patients and settings Children and adults with simple abscesses treated in outpatient clinics or emergency departments.
Data sources Cochrane Central, Medline, Embase and bibliographies.
Outcome measures Percentage of patients with complete resolution of abscess without the need for recurrent incision and drainage, additional antibiotics, or hospital admission within 7–10 days of treatment.
Results We included four trials, consisting of 589 patients in total (428 adults and 161 children). Patients were randomised to one of three antibiotics (cephridine (27), cephalexin (82), or trimethoprim sulfamethoxazole (161)) or to placebo (285), with 34 lost to follow-up or having incomplete data. When given in addition to incision and drainage, systemic antibiotics did not significantly improve the percentage of patients with complete resolution of their abscesses 7–10 days after treatment (88.1% vs 86.0%; OR 1.17 (95% CI 0.70 to 1.95)).
Conclusions When given in addition to incision and drainage, systemic antibiotics do not significantly improve the percentage of patients with complete resolution of their abscesses.
- wounds, infection
Statistics from Altmetric.com
Introduction
A large number of patients present to the emergency department (ED) each year with a skin abscess, and this number is rising. A study of the national epidemiology of cutaneous abscess conducted between 1996 and 2005 found that the number of ED visits for abscesses rose from 1.2 to 3.3 million, which was considerably greater than the rise in total ED visits during the study period.1 While incision and drainage of abscesses is considered the standard care, the role of adjunctive antibiotics in simple abscesses remains unclear.2 Based on prior studies, antibiotics are prescribed in roughly half the ED patients with abscesses, with 51% of the antibiotic regimens including trimethoprim-sulfamethoxazole active against community-associated methicillin-resistant Staphylococcus aureus.1 ,3 There is a large degree of variability in use of antibiotics, with some centres using antibiotics in all patients,4 while others use them only in a minority of patients. There have been several small observational studies and clinical trials that have evaluated the potential benefits of adjunctive systemic antibiotics in patients with simple abscess though the results have been inconclusive. Several large ongoing National Institutes of Health (NIH)-sponsored clinical trials are evaluating the need for adjunctive antibiotics in patients with simple abscess. However, it is unclear when these results will become available.
The lack of clear-cut evidence supporting routine administration of adjunctive systemic antibiotics in patients with simple abscesses prompted us to conduct a meta-analysis of interventional trials comparing the effects of antibiotics and placebo on outcome after incision and drainage of simple cutaneous abscesses.
Methods
Data selection and extraction
We conducted a systematic search of the MEDLINE, Embase, Scopus databases and the Cochrane registry of clinical trials (last accessed 15 Dec 2012) using the terms ‘abscess’, ‘antibiotics’, ‘clinical trial’ and ‘outcome’. We performed an additional search using Google Scholar and a list of bibliographies. We also searched trial registries and abstracts of major emergency medicine (EM) congresses. We included all studies that were placebo-controlled, randomised trials that compared any oral antibiotic (intervention) with a placebo (comparator) in ED patients after incision and drainage of their abscesses (patients) and provided outcome data on clinical cure (outcomes). We excluded animal trials and crossover trials. Two investigators independently screened studies by title and abstract to evaluate whether the trial fitted the inclusion criteria.
Two authors extracted data independently on a predefined data extraction form. A two-by-two summary table was completed for each outcome and for each trial, summarising the number of patients who experienced the event or outcome for each group. These data were double-checked. If there was any disagreement, then the source data were evaluated jointly. The primary outcome was clinical cure at 7 or 10 days, and a secondary outcome was abscess recurrence at 30 or 90 days.
For the randomised trials, two authors independently collected information from all studies to assess the risk of bias using the Cochrane risk of bias tool.5 We collected information on random sequence allocation (selection bias), allocation concealment (selection bias), blinding of participants and personnel (performance bias), blinding of outcome assessment (detection bias), incomplete outcome data (attrition bias), selective reporting (reporting bias), and any other obvious bias.
We assigned ‘low risk’, ‘high risk’ or ‘unable to determine’ to each item of the Cochrane risk of bias tool. Data are reported in accordance with the PRISMA guidelines for systematic reviews.6 Since this was a meta-analysis of published articles, it was exempt from institutional review board (IRB) review.
Statistical analysis
For each randomised trial and the aggregate analysis, we used the OR as the summary measure of association. We evaluated statistical heterogeneity among studies using Cochrane Q and I2 statistics.7 We evaluated publication bias by means of visual inspection of the funnel plot.8 ,9 Data were analysed using REVMAN5 using weighted analysis where the weights were the inverse of the variance of the effects estimates.5 All reported p values are two-sided, and p < 0.05 was considered to be statistically significant.
Results
A total of 106 studies were identified, of which 102 were excluded (retrospective, observational, complicated abscess, lack of placebo) so that four trials were kept for analysis. All these were randomised, placebo-controlled trials in ED patients with simple non-complicated abscesses. Risk of bias was determined to be low based on the criteria in REVMAN5 (table 1).
Risk of bias
The four randomised trials included 589 patients in total (428 adults and 161 children). Patients were randomised to one of three antibiotics (cephridine (27),10 cephalexin (82),11 or trimethoprim sulfamethoxazole (161)12 ,13) or to placebo (285) with 34 lost to follow-up or having incomplete data. Three studies used clinical cure at 7 days,10 ,11 ,13 and one study used clinical cure at 10 days as their primary end point.12 When given in addition to incision and drainage, systemic antibiotics did not significantly improve the percentage of patients with complete resolution of their abscesses 7–10 days after treatment (88.1% (95% CI 85.7 to 92.9) vs 86.0% (95% CI 79.6 to 88.1); difference, 2% (95% CI −4% to 7%); OR 1.17 (95% CI 0.70 to 1.95)) (figure 1). There was no significant heterogeneity among trials (p=0.30; I2=18%). The funnel plot did not reveal any publication bias. Limiting the analysis to only those studies with a 7-day endpoint had no impact on the results.
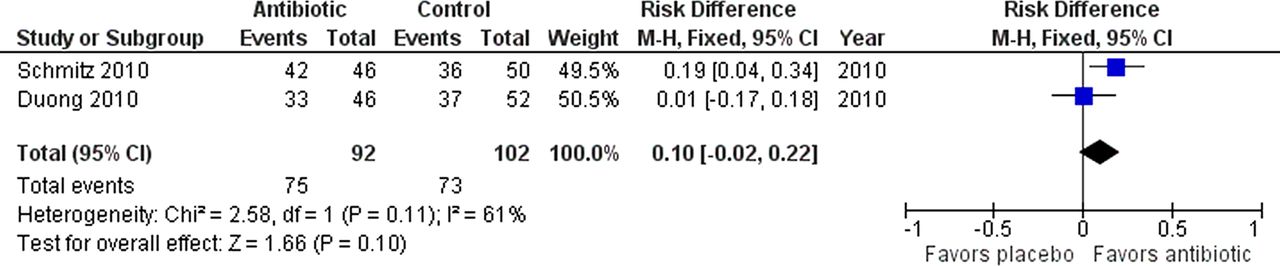
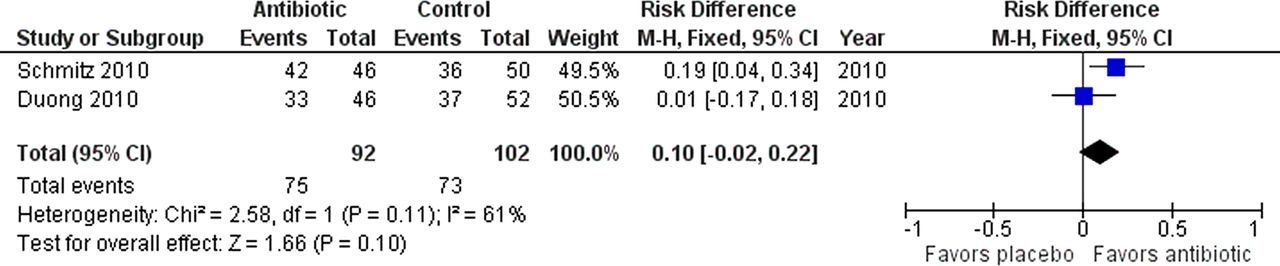
Follow-up beyond the first 7–10 days was performed in two of the trials, at 30 and at 90 days after incision and drainage.12 ,13 When given in addition to incision and drainage, systemic antibiotics did not significantly increase the percentage of patients without abscess recurrence 30–90 days after treatment (81.5% (95% CI 73.6 to 89.5) vs 71.6% (95% CI 62.8 to 80.3); difference 10% (95% CI −2 to 22), OR 1.74 (95% CI 0.88 to 3.45)) (figure 2).

Forest plots for 7–10-day cure rates.
{kind=link}
{kind=link}
Forest plots for 30–90-day recurrence rates.
Discussion
This systematic review and meta-analysis reveals that use of adjunctive oral antibiotics after incision and drainage of simple cutaneous abscesses in the ED does not increase the early 7–10-day cure rate, nor does it reduce the rate of abscess recurrence 30–90 days after incision and drainage. Individually and collectively, the clinical trials included in this systematic review showed no advantage of antibiotics over placebo.
The results of this meta-analysis are in agreement with the recent clinical practice guidelines by the Infectious Diseases Society of America for the treatment of methicillin-resistant Staphylococcus aureus infections in adults and children. These guidelines recommend incision and drainage alone for simple abscesses with systemic antibiotics only for severe or extensive disease, rapid progression in the presence of associated cellulitis, signs and symptoms of systemic illness, associated comorbidities or immunosuppression, extremes of age, abscess in an area difficult to drain, associated septic phlebitis, and lack of response to incision and drainage.2
Only two of the included trials involved an antibiotic with specific activity against most strains of community associated methicillin resistant staphylococcus aureaus (CA-MRSA), which is responsible for more than half of all skin and soft tissue infections in a recent multicenter ED-based study.14 Even when the meta-analysis is limited to the latter two studies, there is no statistically significant difference in 7–10 cure rates (mean difference 6.2%, 95% CI −1.3 to 13.7). Empiric antibiotics, if prescribed, should demonstrate in vitro activity against CA-MRSA. Trimethoprim sulfamethoxazole, clindamycin, and tetracycline have all demonstrated in vitro activity against >90% of over 300 isolates tested in the 2008 US ED-based surveillance study.15 If the abscess is associated with significant cellulitis, or cannot be distinguished from cellulitis, consideration should be given to adding an antibiotic active against Streptococcus pyogenes, which is responsible for most cases of cellulitis without abscess.
Limitations
Our study has several limitations. First, it is limited to four randomised clinical trials including less than 600 patients. Thus, it may have been underpowered to detect small yet clinically significant differences in outcomes. Second, longer-term follow-up was only performed in two of the studies which further increased the risk of a type II error. Third, most of the studies lacked enough detail to determine the effect of confounding variables, such as adequacy of drainage and compliance with assigned treatments.
In conclusion, this meta-analysis of ED patients with simple abscesses indicates that adjunctive oral antibiotics do not increase the cure rate or recurrence rates after incision and drainage.
References
Footnotes
-
Contributors The study was conceived by AJS, and data analysis was by HCT and AJS. AJS wrote the first draft and all authors reviewed and approved the final manuscript.
-
Competing interests None.
-
Ethics approval IRB.
-
Provenance and peer review Not commissioned; internally peer reviewed.