Article Text

Abstract
Objective To evaluate the effectiveness of exercise and physical activity (PA) promotion on cardiovascular fitness, muscle strength, flexibility, neuromotor performance (eg, balance) and daily PA in people with rheumatoid arthritis (RA), spondyloarthritis (SpA) and hip/knee osteoarthritis (HOA/KOA).
Methods systematic review (SR) and meta-analysis (MA) were performed searching the databases PubMed/Medline, CENTRAL, Embase, Web of Science, Emcare and PsycInfo until April 2017. We included randomised controlled trials (RCTs) in adults (≥18 years) with RA, SpA and HOA/KOA, investigating the effects of exercise or PA promotion according to the public health PA recommendations by the American College of Sports Medicine. The time point of interest was the first assessment after the intervention period. If suitable, data were pooled in a MA using a random-effects model presented as standardised mean difference (SMD).
Results The SR included 63 RCTs, of which 49 (3909 people with RA/SpA/HOA/KOA) were included in the MA. Moderate effects were found of aerobic exercises and resistance training on cardiovascular fitness (SMD 0.56 (95% CI 0.38 to 0.75)) and muscle strength (SMD 0.54 (95% CI 0.35 to 0.72)), respectively, but no effect of combined strength/aerobic/flexibility exercises on flexibility (SMD 0.12 (95% CI -0.16 to 0.41)). PA promotion interventions produced a small increase in PA behaviour (SMD 0.21 (95% CI 0.03 to 0.38)).
Conclusion Exercises and PA promotion according to public health recommendations for PA improved cardiovascular fitness, muscle strength and PA behaviour, with moderate effect sizes in people with SpA, RA and HOA/KOA.
Trial registration number CRD42017082131.
- rehabilitation
- rheumatoid arthritis
- spondyloarthritis
- osteoarthritis
- knee osteoarthritis
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
What is already known about this subject?
There are public health recommendations for physical activity in healthy adults of all ages. Exercise is a cornerstone for the management of rheumatoid arthritis (RA), spondyloarthritis (SpA) and hip/knee osteoarthritis (HOA/KOA), but exercise interventions may not meet these recommendations.
What does this study add?
Exercise interventions according to the public health recommendations in appropriate dose (frequency, intensity, time, type, volume, progression) is effective on cardiorespiratory fitness and muscle strength in people with RA, SpA and HOA/KOA.
Counselling-based physical activity promotion interventions according to the public health recommendations effectively change physical activity behaviour in people with RA, SpA and HOA/KOA.
There is a knowledge gap concerning the effects of flexibility and neuromotor exercises in people with RA, SpA and HOA/KOA.
How might this impact on clinical practice?
Exercise and physical activity promotion according to the public health recommendations is effective and should be an integral part of standard care throughout the course of the disease in people with RA, SpA and HOA/KOA.
Physical activity (PA) is defined as 'any bodily movement produced by skeletal muscles that result in energy expenditure'1 2 above resting (basal) levels. PA encompasses exercise, sports and physical activities, done as part of daily living, occupation, leisure and active transportation.3 Exercise is a subcategory of ‘physical activity that is planned, structured, and repetitive and (that) has as a final or intermediate objective to improve or maintain one or more dimensions of physical fitness’.1 In contrast, therapeutic exercises are specific exercises meant to address particular functional health problems.
WHO recommends that adults, including elderly or people with chronic conditions, perform at least 150 min of moderate-intensity or 75 min of vigorous-intensity PA a week (or a combination of it) and additional muscle strengthening activities involving major muscle groups on at least 2 days a week.4 The American College of Sports Medicine (ACSM) recommends additional regular performance of flexibility and neuromotor activities such as balance or agility on at least 2 days a week.3 Accordingly, exercising in the four dimensions cardiovascular fitness, muscle strength, flexibility and neuromotor performance is recommended. The absolute energy demands of PA can be estimated by MET (metabolic equivalent of task)5: PA like walking 5 km/h is described by 3.2 METs, which is classified as a moderate-intensity activity; PA like jogging 9 km/h is described by 8.8 METs. Following Garber and colleagues,3 the use of absolute measures may however be misleading because personal factors like weight, sex or fitness level are not considered. For this reason, a relative measure of intensity (ie, the energy costs relative to the individual maximal capacity) like %METmax, %HRmax or perceived exertion is more appropriate. Moderate exercise is defined as 64% to 76% of the maximum heart rate (%HRmax), and vigorous exercise is defined as 77% to 95% HRmax. Furthermore, there is evidence that shorter (eg, 30 min) vigorous intensity (≥6 METs) of cardiovascular exercise is associated with a greater reduction of cardiovascular risk6 and lower mortality rate in the general population7 than longer (eg, 60 min) moderate intensity (3–6METs) cardiovascular exercise.
The dose–response relationship between daily PA and health benefits was proven; by exceeding the minimum recommended amount of PA, the results regarding improvement of fitness, reduction of risk factors of chronic conditions and prevention of unhealthy weight gain are enhanced.3
The evidence for the benefits of regular PA in healthy people is overwhelming.8 9 The benefits of PA are obvious in people with rheumatoid arthritis (RA),10 spondyloarthritis (SpA)11 and hip/knee osteoarthritis (HOA/KOA),12 and exercise is the cornerstone of the European League Against Rheumatism (EULAR) recommendations for the non-pharmacological disease management of 1 RA14, axial SpA15 and HOA/KOA.⇓ No specific recommendations on PA were available yet; therefore, in 2016, the EULAR project ‘recommendations for PA in people with inflammatory arthritis and osteoarthritis’16 was started. The task force, developing the recommendations, agreed that RA and SpA as predominant inflammatory arthritis (iA) conditions, and HOA/KOA as most relevant for PA recommendations represented the field of iA and OA, respectively. The resulting ‘2018 recommendations for PA’ provide four overarching principles and 10 recommendations which suggest PA as an integral part of standard care throughout the course of disease in people with RA, SpA and HOA/KOA, given its effectiveness, safety and feasibility.
The recommendations for PA in people with RA, SpA and HOA/KOA may constitute a bridge between arthritis-specific exercises and public health recommendations for PA. They are also important because clinical practice shows that patients and clinicians may still believe that PA and exercising according to public health recommendations3 4 is potentially harmful and accelerate disease progression. Furthermore, the best strategy for the promotion of daily PA is still a matter of debate and a challenge for health professionals. However, there is evidence for the effectiveness of behaviour change techniques (BCTs) in PA promotion.17 18
The EULAR Standardized Operating Procedures (SOPs) for the development of recommendations19 demand a systematic review (SR) of the literature with qualitative and if possible quantitative analysis, that is, a meta-analysis (MA), to inform the development of recommendations where appropriate. The aim of this paper is to report in detail on the MA that was performed to answer the question on the effectiveness of PA interventions in people with RA, SpA, HOA and KOA as basis for the EULAR PA recommendations.
This SR included only studies that met the dose for effective PA according to the public health recommendations for PA as provided by the ACSM for at least one dimension of exercise.
Methods
Design
This study was conducted following the Cochrane Guidelines20 as requested by the EULAR SOP19 and the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) analysis grid. The study was registered in PROSPERO (CRD42017082131; https://www.crd.york.ac.uk/ PROSPERO/).
Selection criteria
Included were randomised controlled trials (RCTs) on patients with RA, SpA and HOA or KOA, where the intervention of interest met the dose of the public health recommendations for effective PA as provided by ACSM for at least one dimension of exercise compared with any intervention not meeting the ACSM recommendations, such as low-dosed exercise, home exercises, attention control, usual care and waiting list. Further, for the inclusion in the SR, studies needed to investigate
the effect of cardiovascular exercises on cardiovascular fitness,
or
the effect of muscle strength exercise on lower limb muscle strength,
or
the effect of flexibility exercises on flexibility,
or
the effect or neuromotor exercise on neuromotor performance,
or
the effect of a physical activity promotion strategy on the amount of daily PA in people with RA, SpA, HOA or KOA.
The MA involved those studies with the most frequently used proxy for cardiovascular fitness (eg, VO2max, watts both assessed on a treadmill/bicycle ergometer), muscle strength (of the lower limb like M.quadriceps femoris), flexibility (eg, passive/active range of motion (ROM), Bath Ankylosing Spondylitis Metrology Index) and PA (eg, questionnaire, accelerometer). The time point of interest was the first assessment after the intervention period.
Search strategy
Given the presumably high number of available literature, we chose a pragmatic approach: We first searched for key MA or SR including RCTs and, second, updated the yield with recently published RCTs that investigated the effectiveness of PA interventions in adults with RA/SpA/HOA/KOA according to the inclusion criteria described before. The SR was performed in PubMed/Medline, Cochrane Library, Embase, Web of Science, Emcare and PsycInfo, using both MeSH terms and freetext, covering the time frame until April 2017.
No language restrictions were applied. No additional search for grey literature or ongoing studies or unpublished data was conducted. Reference lists of included studies were scanned, and experts in the field of RA (EH), SpA (HD), HOA/KOA (CBJ) and behaviour change (KK) were consulted identifying relevant missing studies. The search strategy for PubMed/Medline is provided in online supplementary file 1. A-KRO and KN screened first the abstracts of all identified records and second assessed full-text papers fulfilling the inclusion criteria.
Supplemental material
Risk of bias assessment
The risk of bias assessment included the methodological domains: random sequence generation (selection bias), allocation concealment (selection bias), blinding of participants (performance bias), blinding of outcome assessment (detection bias), incomplete data (attrition bias), selective bias (reporting bias) and other potential bias. These criteria were judged as ‘high risk’, ‘low risk’ or ‘unclear risk’ as described by the Cochrane Handbook for Systematic Reviews of Interventions.20 Due to the vast number of studies included, we used a pragmatic approach. If a previous SR or MA had coded included studies for risk of bias, then these ratings were used here, after being spot-checked by the first author (A-KRO). When no previous review or meta-analyses had assessed risk of bias with the Cochrane risk of bias assessment tool, risk of bias rating was performed by two independent assessors (A-KRO, CH). If agreement was not achieved, a third review author (KN) made a final decision. Publication bias was investigated as small study bias and assessed by visual inspection of the funnel plot asymmetry.
Data extraction and management
The data extraction was performed by one reviewer (A-KRO) and verified by double reading (CBJ). In studies with more than one intervention group, the intervention groups were pooled if there were only small differences in the intervention (eg, walking or swimming as aerobic exercise intervention). Some authors were contacted to obtain unreported data.
Synthesis of data
Applying the PRISMA procedure, this MA focused on the quantitative analysis. The effects of PA on cardiovascular fitness, muscle strength and flexibility were calculated as the standardised mean difference (SMD), allowing for pooling the results of the various outcomes assessed in individual trials. The SMD was estimated as the difference between the postintervention scores in the intervention and control groups divided by the pooled SD. The SD was extracted or estimated from the SE, the 95% CI, the p value, IQR or other methods recommended by the Cochrane Collaboration.20 The SMD was clinically interpreted as originally proposed by Cohen.21 An SMD of 0.2 was considered small, an SMD of 0.5 was considered moderate (and would be recognised as clinically important) and an SMD equal to 0.8 was considered large.20 This estimate of the effect size is slightly biased, overestimating the effect size of small studies, and a correction factor was applied to convert the effect size to Hedges’s g. Meta-analyses using a random-effects model were applied. Heterogeneity was tested using the Q-test and was further quantified as the I2 statistic22 measuring the proportion of variation (ie, inconsistency) in the combined estimates due to between-study variance.23 An I2 value of <40% means low inconsistency between the results of individual trials, and an I2 value of 100% means maximal inconsistency. All statistical analyses were performed in Stata V.15 (StataCorp, College Station, Texas, USA).
Results
Study selection and study characteristics
The literature search revealed 3460 records; 237 of these were screened in full text (figure 1). A total of 174 studies were excluded due to unclear or insufficient dose (n=117), inappropriate study design (n=11), therapeutic exercise intervention (n=9), no between-group difference reported (n=12), joint replacement during intervention (n=5) and no appropriate outcome (n=20). The SR comprised 63 RCTs11 24–87 (two RCTs were reported by two papers each33 49 78 82) published between 1985 and 2017, of which 49 RCTs were included in the MA. The sample size of these studies ranged from 16 to 222 participants; overall, a total of 3909 participants (mean age (SD) 56.2 (9.6) years) were included in the MA (1049 people with RA, 508 people with SpA, 1855 people with KOA and 497 people with HOA). The interventions lasted between 4 and 104 weeks, and all studies assessed before and after the intervention. However, further assessment time points were heterogeneous; six studies (13%) performed one or several follow-ups, up to 29 months.37 52 54 66 81 83 No detrimental effects of PA were reported in any study. Study characteristics of all studies included in the SR are provided in online supplementary table 1; interventions with assessments and outcomes are described in online supplementary tables 2–5.
Supplemental material
Supplemental material

Preferred Reporting Items for Systematic Reviews and Meta-Analysis flow chart describing the detailed selection process.
Risk of bias within studies
Online supplementary figures 6–10, describe the Cochrane risk of bias assessment. Ratings of 32 studies were adopted from existing SRs/MAs and spot-checked by the first author.12 18 88–90 The remaining articles were coded for risk of bias. Two RCTs were rated as low risk of bias for all items.30 37 Randomisation was performed according Cochrane criteria20 in 44 (67%) RCTs. The allocation concealment was ensured in 31 (47%) RCTs. The blinding of participants was assured in 8 RCTs (12%), the blinding of the outcomes assessment in 30 (46%) RCTs. The risk of incomplete data was low in 49 (75%) RCTs. In 32 (48%) RCTs, a study protocol was available, with corresponding published data, resulting in a low risk for selective reporting.
Effects on cardiovascular fitness
Sixteen RCTs investigated the effect of aerobic exercise on cardiovascular fitness (online supplementary table 2), including 1326 participants with a mean (SD) age of 51.4 (7.2) years. The MA showed a moderate effect of SMD 0.56 (95% CI 0.38 to 0.75) (figure 2). The overall heterogeneity of study effects was moderate (I2=42.2%); the funnel plot (online supplementary figure 11) showed an asymmetry, indicating a risk of small study bias.
Supplemental material
Supplemental material
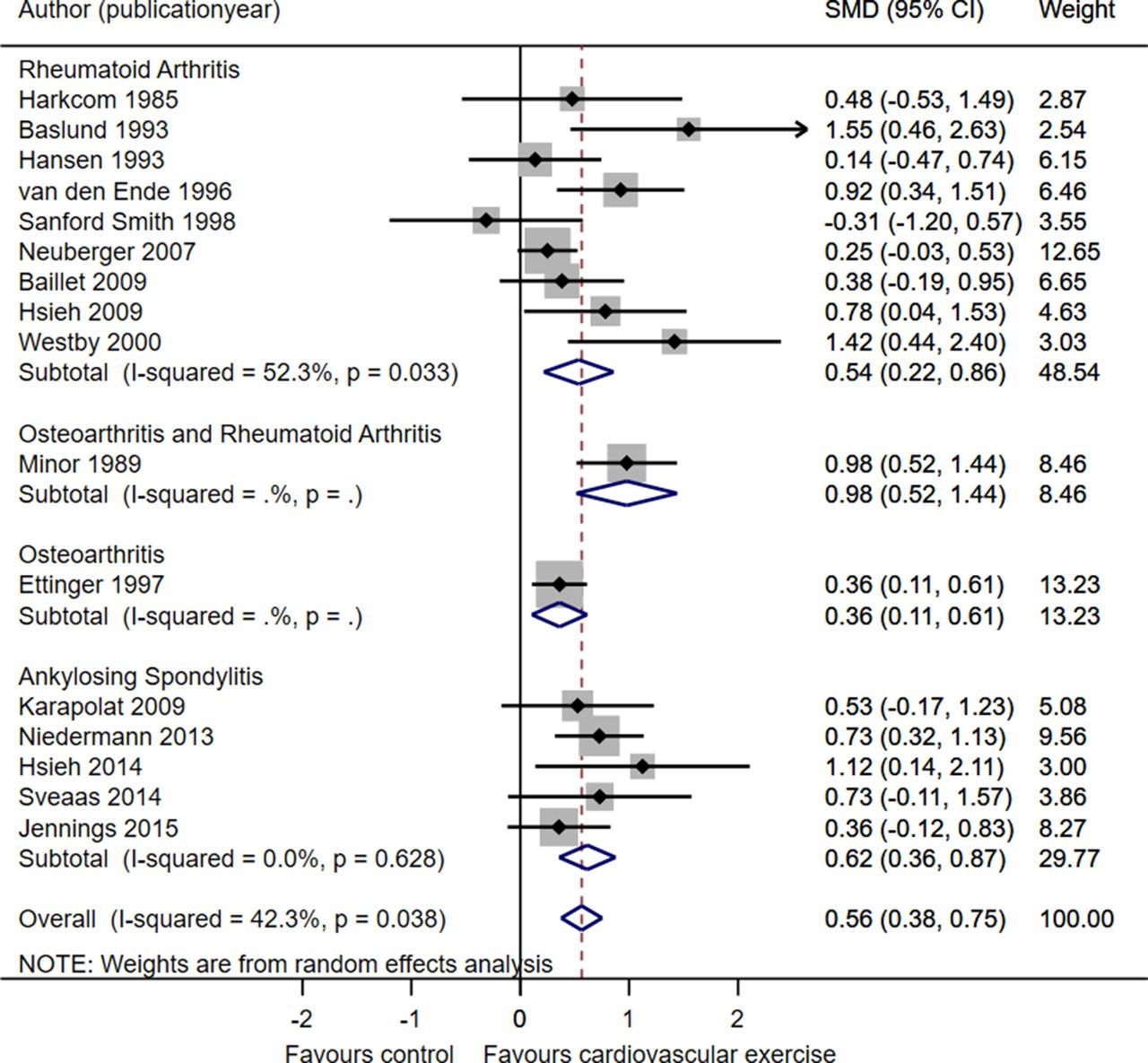
Forest plot showing the results of the meta-analysis on the effect of aerobic exercise on measured on VO2max in people with rheumatoid arthritis, spondyloarthritis and hip/knee osteoarthritis. SMD, standardised mean difference.
Effects on muscle strength
Thirty-one RCTs investigated the effect of muscle strength exercises on lower limb muscle strength in people with RA or HOA/KOA (online supplementary table 3), of which 28 provided data on M.quadriceps femoris strength. The measurement (60°/sec, 90°/sec) and units (Nm, kp, kg, N, S/kg) varied between the studies; therefore, analyses were performed on SMD. Three RCTs were not included as they reported data in median and range.43 75 91 Although these data could be recalculated into mean and SD, this may lead to imprecise data given the small sample sizes in these studies. If strength was described for both legs, values for the affected leg/joint were included in the analysis. If strength was measured in different positions, the velocity of 60°/sec was preferred for the MA. Twenty-five RCTs, including 936 participants with a mean (SD) age of 61.5 (5.0) years, were included in the MA, which showed a moderate effect of muscle strength exercise on M.quadriceps femoris strength with an SMD 0.54 (95% CI 0.35 to 0.72; figure 3) with substantial heterogeneity (I2=67%). The funnel plot shows minor asymmetry for both RA and HOA/KOA (online supplementary figure 12), thus the analyses might slightly overestimate the effect for both RA and HOA/KOA.
Supplemental material

Forest plot showing the results of the meta-analysis on the effect of strength exercise on M.quadriceps femoris in people with rheumatoid arthritis and hip/knee osteoarthritis. SMD, standardised mean difference.
Effects on flexibility
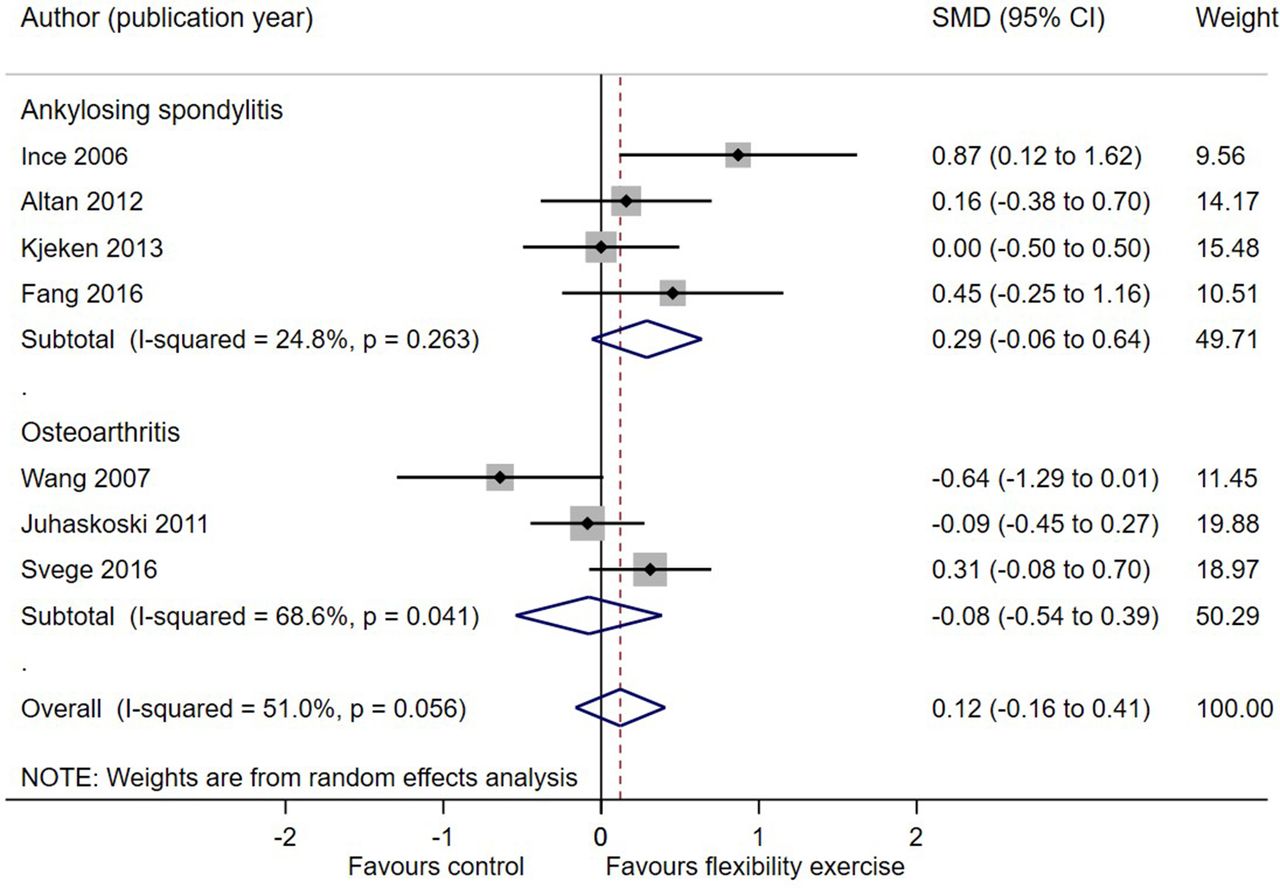
Eight RCTs investigated the effect of flexibility exercises (ROM, stretching) combined with strength or aerobic exercises compared with no exercise or usual care, and measured the effect on ROM (passive or active) or the Bath Ankylosing Spondylitis Mobility Index. One RCT was not included in the MA as data was presented as median and range.71 None of the RCTs compared flexibility exercises alone with no exercises (online supplementary table 4). The MA of the seven RCTs, including 477 participants with a mean (SD) age of 49.3 (15.2) years, showed no effect of the exercises combination on flexibility either for RA or HOA/KOA showing an overall SMD 0.12 (95% CI -0.16 to 0.41) (figure 4). The overall heterogeneity of study effects was moderate (I2=31.1%). Publication bias was not evaluated due to the sparse number of included studies, especially when stratifying on patient group (HOA/KOA and SpA) in the MA.20
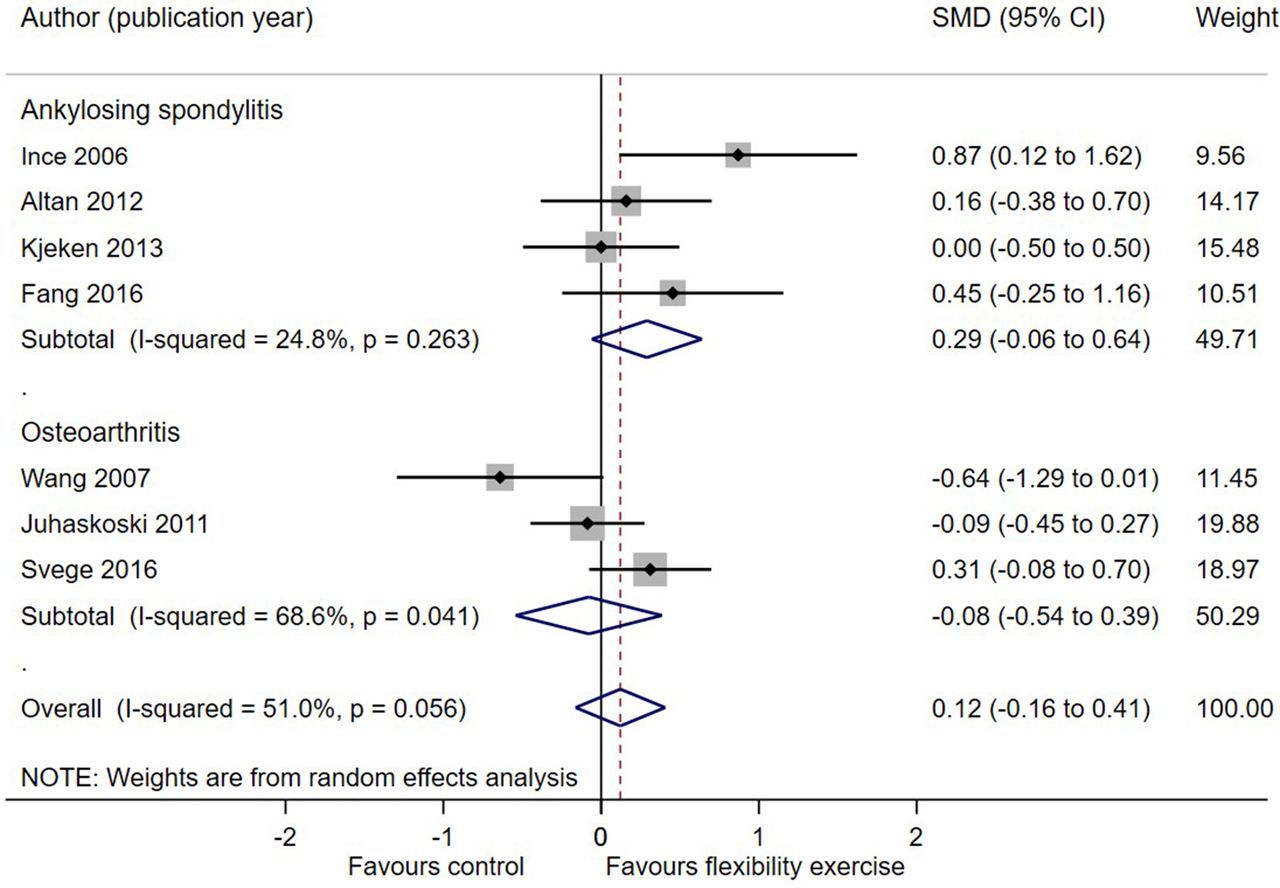
Forest plot showing the results of the meta-analysis on the effect of flexibility exercises combined with strength or aerobic exercises on flexibility in people with ankylosing spondylitis and hip/knee osteoarthritis. Flexibility was measured as active or passive range of motion, and using the Bath Ankylosing Spondylitis Mobility Index. SMD, standardised mean difference.
Effects on neuromotor performance
Studies evaluating neuromotor performance were scarce. Da Silva and colleagues36 showed that a 16-week neuromotor exercise programme had a statistically positive effect in neuromotor performance in 91 people with RA, evaluated with Berg Balance Scale, Tinettis Test and Timed-Up-and-Go Test. Four RCTs in people with KOA who performed strength exercises, evaluated neuromotor performance with the step test for standing balance, reposition error of the knee, Berg Balance Scale and one leg standing time with eyes open. Two RCTs showed a positive effect63 92; two found no effect.74 93 Røgind and colleagues71 investigated the effect of a programme combining strength, stretching, mobility and balance exercises on postural sway, but found no effects.
Effects on daily PA
Eleven RCTs investigated the effect of a daily PA promotion intervention on daily PA (online supplementary table 5) evaluated by accelerometer or questionnaire. In six RCTs, counselling based on BCTs was an essential component of the intervention.30 31 34 58 61 69 Three RCTs did not include a counselling strategy as part of the intervention46 56 70 and two studies described data with percentages33 49 78 82 and were therefore excluded from the analysis. The MA of the six studies, including 694 participants with a mean (SD) age of 59.5 (9.5) years, showed a small effect SMD 0.21 (95% CI 0.03 to 0.38) (figure 5) with no heterogeneity (0%) and no small study bias (online supplementary figure 13).
Supplemental material

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest plot showing the results of the meta-analysis on the effect of physical activity promotion strategies including counselling. SMD, standardised mean difference.
Discussion
The four MAs overall included 49 studies with 1049 people with RA, 508 people with SpA, 497 people with HOA and 1855 people with KOA. Moderate short-term effects of aerobic and muscle strength exercises on cardiovascular fitness and muscle strength in people with RA, SpA and HOA/KOA were shown. No studies on flexibility exercises alone were found, whereas flexibility exercises combined with muscle strength or aerobic exercise had no effect on flexibility. PA had no detrimental side effects like increased disease activity in any exercise dimension. PA promotion with counselling based on BCTs showed a small beneficial effect on daily PA, which has been shown to be a strong mediator for further health benefits.8 9 However, this MA did not evaluate the effects of increased daily PA on health benefits. Overall, this MA confirms the increasing evidence for the multiple benefits of exercise in people with RA, SpA and HOA/KOA, and indicates that PA promotion interventions can increase daily PA within these individuals.
In this MA, we reported the effectiveness estimates for each PA dimension over the three conditions based on the effectiveness data available in the primary studies. Exercise interventions are effective if they achieve a physiological response, such as increased flexibility, muscular strength and cardiovascular fitness, which is determined by the right intervention in its right dose, as well as patient adherence.94 Only seven RCTs, included in the MA (13%), reported (minor) adverse events related to exercise like transient increased pain.30 38 65 77 81 85 92 Our findings regarding the safety of exercise and PA promotion interventions are in line with the literature.3 Even a small to moderate beneficial effect of exercise on joint damage, inflammation and symptoms (pain, stiffness, joint tenderness) was found.89 Bischoff and Roos95 showed that aerobic and strength exercise was equally effective regarding pain and function in people with HOA/KOA. Indeed, the effectiveness of interventions cannot be appraised without taking account to feasibility. The feasibility of interventions can be evaluated by adherence to the intervention or the study protocol (reported as attendance rate). However, (self-)reported adherence to intervention might be overestimated due to recall bias or social desirability.96 For aerobic exercise interventions, 75% of the MA-included studies reported an attendance rate varying between 48% and 100%; for muscle strength exercises, 60% of the MA-included studies reported an attendance rate between 49% and 96%. Attendance rate tends to decline over time,38 42 and the compliance between those with supervised and home exercises seems to vary.47 60 This information underlines that a low compliance rate is one of the most compelling challenges for exercise and PA interventions. Long-term adherence implies a change in lifestyle, which can be supported by interventions based on BCTs.18 97
This MA was based on studies that followed the public health recommendation for PA according to ACSM3 and thus achieved the minimal dose for effective PA interventions. The ACSM98 provide clear recommendations regarding frequency and type of exercise in people with arthritis. Cardiovascular training was performed with no-impact sports like (Nordic) walking,68 dance,86 cycling76 or water-based48 exercising. The recommended intensity varies from moderate to vigorous,3 but also high-intensity training up to 90% of the predicted maximal heart rate or 80% one-repetition-movement appears to be effective and feasible in people with RA.60 83 99 Flexibility exercises were performed as usual care or combined part of the intervention. Most included studies investigated (semi)supervised exercise interventions. ‘Booster strategies’ like phone calls,33 34 47 82 devices (eg, pedometer,34 46 wearable56 61), home visits,27 38 log book,34 47 86 100 web-based instructions,49 written material48 70 86 and visual instructions (eg, video70) were reported. The interventions were always provided by physiotherapists, except in three studies (Pilates trainer,24 physician,76 physiatrist80). Only if adherence to the FITT-VP components of the intervention (frequency, intensity, time, type, volume and progression of exercise) is given and reported the best possible training effect can be achieved and the individual goal on physical performance level can be reached.101 The initiation and maintenance of PA are both challenging and meet different general and disease-specific barriers and facilitators.102–105 This highlights the need for further development in promising strategies, such as BCTs for the promotion of a long-term active lifestyle in people with RA, SpA and HOA/KOA. However, starting and maintaining regular exercise in all four dimensions is difficult, even for healthy people. Therefore, it is important to pinpoint that the public health recommendations for PA3 state that exercise below the recommended levels may still be beneficial for people not able or not willing to fulfil the recommended amount of PA.
Strengths and limitations
To our knowledge, this is the first MA gathering the current evidence on the effectiveness of exercising according to the ACSM principles3 with regard to the dimensions and dose for exercise in the three rheumatic conditions RA, SpA and HOA/KOA. The aim of this MA was to evaluate the overall effect of exercise and PA promotion, and we do not have evidence to suspect heterogeneity in treatment response among these conditions. However, a disease-specific analysis could be beneficial.
The vast variability of used assessments and scales led us to indirect comparisons. Our analysis illustrates that a consensus on assessments in the field of PA could help to launch more research with comparative outcomes and findings. Gates and colleagues106 described a consensus how to facilitate the comparison of data between heterogeneous studies in research on PA in HOA/KOA. One of the important points was to decide on MET minutes per week as a key method to assess daily PA and defined minimal requirements for future studies. Being aware of the indirect comparisons, the analyses were a good basis for the task force to decide on PA recommendations for people with RA, SpA and HOA/KOA. More studies with a larger number of participants and similar assessments are needed to clearly decide on the long-term effects of exercise, as the overall aim of PA promotion is a change in long-term life style. Long-term supervised exercises seem to be more effective than short-term exercises88 107; however, the intervention duration and setting was not part of this analysis.
It is a limitation that only one reviewer screened the abstracts and decided on unclear abstracts together with a second reviewer, which is not fully in line with standard procedures of a SR.108 However, we applied a double check by experts to ensure that no relevant studies were missed.
Conclusion/clinical implication
Physical activity according to public health recommendations following the ACSM principles3 show moderate effectiveness on cardiorespiratory and muscle strength as well as PA promotion interventions based on counselling in people with with RA, SpA and HOA/KOA. No evidence was found for the effects of flexibility exercises and almost no literature was available evaluating neuromotor exercises. Many studies had to be excluded due to poor reporting on the intervention. Future studies should use the TIDieR-checklist109 (Template for Intervention Description and Replication) or CERT110 (Consensus on Exercise Reporting Template) to improve completeness of reporting. This will enable clinicians to implement effective interventions and researchers to replicate or merge findings.
Supplemental material
Supplemental material
Supplemental material
Supplemental material
Supplemental material
Supplemental material
Acknowledgments
We thank Mrs José Plevier, Walaeus Library, Leiden University Medical Center, Leiden, The Netherlands, for supporting our literature search, and Christian Horvath (CH), MSc student at ZHAW for his help in the Cochrane risk of bias assessment. Many thanks to all Task Force Members of the EULAR endorsed project ‘2018 EULAR recommendations for physical activity in people with inflammatory arthritis and osteoarthritis’, who all participated actively in the development of the recommendations and supported the idea of a MA.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- 89.↵
- 90.↵
- 91.↵
- 92.↵
- 93.↵
- 94.↵
- 95.↵
- 96.↵
- 97.↵
- 98.↵
- 99.↵
- 100.↵
- 101.↵
- 102.↵
- 103.↵
- 104.↵
- 105.↵
- 106.↵
- 107.↵
- 108.↵
- 109.↵
- 110.↵
Footnotes
TPMVV and KN contributed equally.
Contributors A-KRO performed the SLR and data extraction, supervised by KN and TPMVV. JS developed the search strategy for all databases. CBJ double-checked data and performed the meta-analysis. A-KRO and KN drafted the manuscript. All authors of this manuscript were members of the EULAR Task Force, except JS, who developed the recommendations for physical activity in people with inflammatory arthritis and osteoarthritis. They revised this manuscript and approved the final version for publication.
Funding The manuscript is part of the EULAR project ‘2018 EULAR recommendations for physical activity in people with inflammatory Arthritis and Osteoarthritis’.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement There are no unpublished data from this study.