Article Text

Abstract
In the 2016 update of the stable chest pain guideline, the National Institute for Health and Care Excellence (NICE) has made radical changes to the diagnostic paradigm that it—like other international guidelines—had previously placed at the centre of its recommendations. No longer are quantitative assessments of the disease probability considered necessary to determine the need for diagnostic testing and the choice of test. Instead, the recommendation is for no diagnostic testing if chest pain is judged to be ‘non-anginal’ and CT coronary angiography (CTCA) in patients with ‘typical’ or ‘atypical’ chest pain with additional perfusion imaging only if there is uncertainty about the functional significance of coronary lesions. The new emphasis on anatomical—as opposed to functional—testing is driven in large part by cost-effectiveness analysis and despite inevitable resource implications NICE calculates that annual savings for the population of England will be significant. In making CTCA the default diagnostic testing strategy in its updated chest pain guideline, NICE has responded emphatically to calls from trialists for CTCA to have a greater role in the diagnostic pathway of patients with suspected angina.
- Advanced cardiac imaging
- Chronic coronary disease
- Cardiac computer tomographic (CT) imaging
Statistics from Altmetric.com
The diagnostic paradigm—as it was in 2010
In the patient with suspected angina, international guidelines1–3 have recommended a careful history to determine the typicality of symptoms (figure 1). Because angina is usually a manifestation of obstructive coronary artery disease (CAD), guidelines have further recommended estimation of disease probability, based on the typicality of symptoms and the age and gender of the patient, to guide the need for diagnostic testing.4 The 2010 National Institute for Health and Care Excellence (NICE) guideline identified no need for testing in patients with a very high (>90%) or very low (<10%) probability of disease because, at these levels of diagnostic certainty, the incremental value is negligible.1 However, for patients in whom disease probability lies between these extremes, recommendations have been for anatomical or functional testing as an aid to decision-making. An abnormal result favours a diagnosis of angina while a normal result often earns the patient reassurance that the pain is non-cardiac in origin.
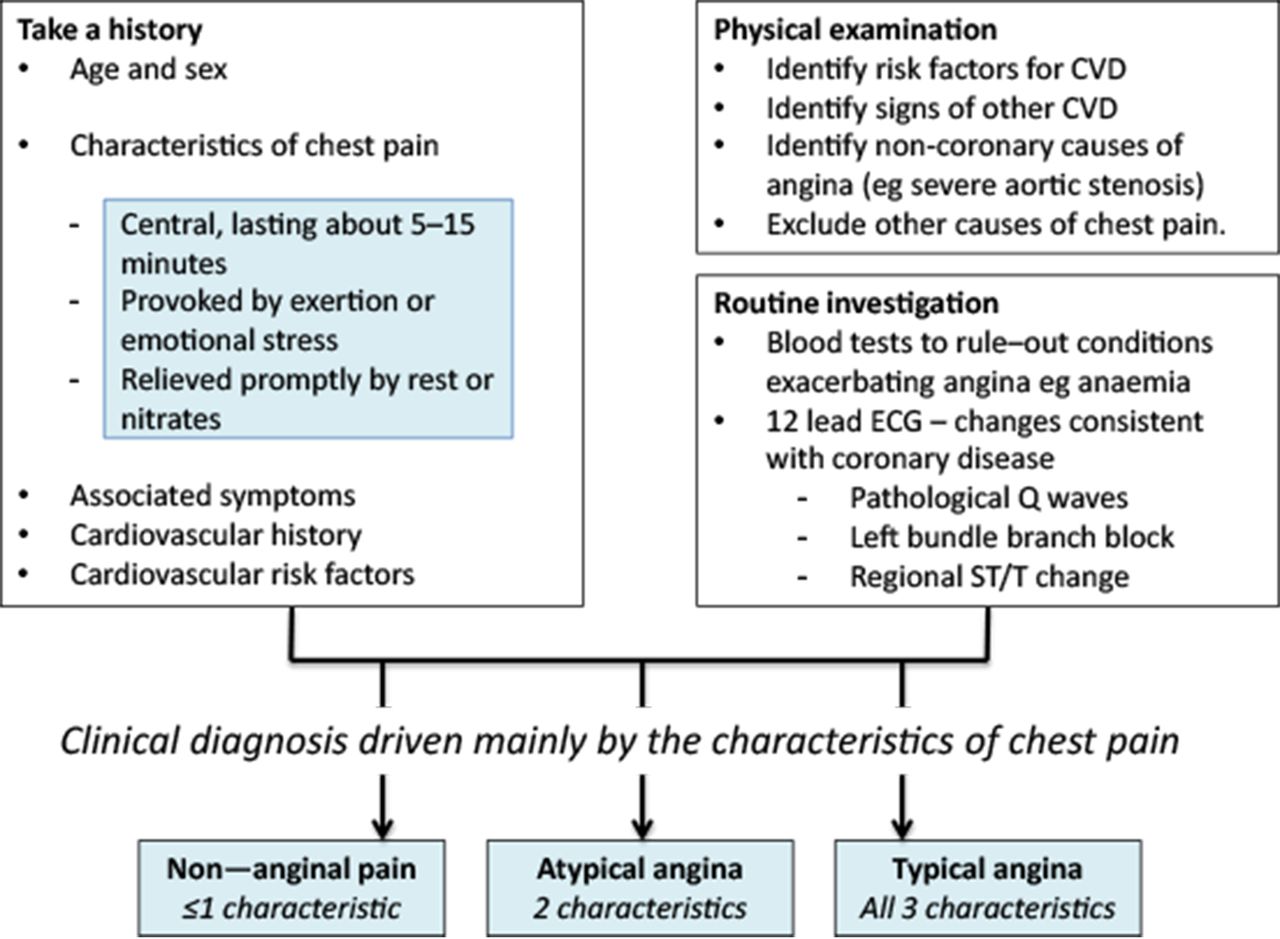
Clinical diagnosis of angina. National Institute for Health and Care Excellence guideline recommendations. CVD, cardiovascular disease.
Is the paradigm still fit for purpose?
The reassurance given to patients with a diagnosis of non-cardiac chest pain may be misplaced. Under-recognition of angina is common and associated with less aggressive treatment escalation and potentially greater risk.5 In chest pain clinic cohorts, such patients account for about one-third of non-fatal myocardial infarctions and coronary deaths during the next 5 years,6 with risk higher in patients managed conservatively without revascularisation.7 This failure to properly identify at-risk individuals is not confined to chest pain clinics, linked electronic health records showing a surge of primary care consultations in the weeks before hospital presentations with acute coronary syndromes.8 Underdiagnosis of at-risk individuals and the missed opportunity to protect them against coronary events is complemented by a parallel tendency towards overdiagnosis, reflected in the large and increasing proportion of patients with chest pain referred for cardiac catheterisation and found to have unobstructed coronary arteries.9 Although ischaemic mechanisms may be driving symptoms in some of these patients, this should not obscure the fact that in most patients angina is a manifestation of CAD, and the diagnostic challenge, therefore, is to determine whether the patient with chest pain has flow-limiting coronary obstructions. This challenge is often not met, questioning whether the guideline-recommended diagnostic paradigm, involving estimates of disease probability refined by the results of diagnostic testing, remains fit for purpose.
How reliable are estimates of disease probability?
Estimates of disease probability in patients with chest pain were first provided by Diamond and Forrester in a simple model incorporating patient age, gender and typicality of symptoms.4 However, there is now considerable uncertainty about the accuracy of these probability estimates. Thus, the Diamond and Forrester disease estimates and their modification in the Duke clinical score10 were developed more than 40 years ago when coronary disease was more prevalent and were derived from angiographic and autopsy populations, further ensuring that disease prevalence, on which the estimates were based, was substantially higher than in contemporary populations attending chest pain clinics. Genders et al 11 recognised this limitation and developed an updated model using more contemporary cohorts that confirmed considerable overestimation of disease probability by Diamond and Forrester, particularly in women. This model shows superior discrimination for obstructive CAD compared with the Diamond and Forrester score as reflected by a c-statistic of 0.752 compared with 0.713,12 but it remains imperfect and because it was developed in angiographic populations is likely to overestimate disease probability in lower risk populations with undiagnosed chest pain.
The failure of diagnostic models to accurately predict disease significantly exaggerates probability estimates, and thereby undermines the validity of the diagnostic paradigm that has been central to guideline recommendations. The exaggeration is not trivial, the CONFIRM (Coronary CT angiography evaluation for clinical outcomes: an international multicenter registry) investigators reporting that the observed prevalence of significant (>50%) obstructive disease in 14 048 patients with suspected angina who underwent CT coronary angiography (CA) was only 18% compared with 51% predicted by the Diamond Forrester disease estimates tabulated in the American Heart Association guideline.13 For 70% stenosis, the observed and predicted prevalence rates (10% vs 42%) showed even wider separation. Similar separation of observed and predicted rates of obstructive coronary disease have been reported for the Duke Clinical Score, a modification of the Diamond Forrester model recommended in the NICE 2010 guideline.14 Now, indirect observations suggest that the Genders updated disease estimates, recommended in the European Society of Cardiology guideline, may be similarly unreliable. Thus, a recent study found that patients with disease estimates as high as 60%–90% (mean 74%) had an annualised coronary mortality rate of only 0.7%.15 This apparent mismatch between predicted disease and observed mortality emphasises the likely unreliability of the disease estimates and the importance of considering prognostic indicators in patients with suspected angina so that those at greatest risk might be identified. The Prognosis In Suspected Angina model based on simple clinical factors available at the initial cardiological assessment has been internally validated in a large chest pain clinic cohort and shows strong associations with coronary mortality (c-statistic 0.83).15 A desktop calculator is available and promises to emerge as an important clinical tool if further validation studies are favourable.
Which diagnostic test?
The non-invasive tests listed in table 1 have found widespread application for the diagnosis of angina. However, the information they provide shows important differences particularly when CTCA is compared with the other tests. CTCA provides direct anatomical evidence of the presence and severity of epicardial CAD, while the other tests provide ‘functional’ information about stress-induced perfusion defects or wall motion abnormalities as evidence of ischaemia caused by obstructive epicardial coronary disease. Functional tests may find additional application in the small but important group of patients with angina in whom the epicardial coronary arteries on anatomical testing are unobstructed.16 17 Stress-induced perfusion defects or wall motion abnormalities in such patients are diagnostically helpful in providing evidence of ischaemia caused by small vessel disease.
Ischaemia testing for diagnosis of CAD: sensitivity and specificity data from meta-analytic reviews
Table 1 shows sensitivity and specificity data for the diagnosis of epicardial CAD from selected meta-analyses for the commonly used non-invasive tests.18–29 Despite variation between individual studies, it is clear that the exercise ECG performs less well than the other diagnostic tests, particularly in terms of its sensitivity for ruling out CAD. Thus, Genders et al, 14 in developing their updated prediction model in a pooled analysis of angiographic cohorts, concluded that ‘the diagnostic value of exercise electrocardiography is limited’. Sekhri et al 30 similarly concluded that the exercise ECG adds little to the routine clinical assessment in determining the prognosis of patients with stable chest pain. NICE echoed these conclusions in its 2010 chest pain guideline, recommending that the exercise ECG should no longer be used to diagnose or exclude stable angina, preferring the other diagnostic tests listed in table 1.31 Although the superiority of these tests compared with the exercise ECG is widely acknowledged the derivation of their diagnostic metrics against an angiographic gold standard is a potential limitation. Thus, although the sensitivity and specificity data can be considered fixed properties of the tests, their clinically relevant positive predictive values (how likely is a patient with a positive test result to actually have the disease?) will be diminished in low-risk chest pain clinic populations, increasing the risk of false-positive diagnosis and unnecessary cardiac catheterisation.
Anatomical testing
This review has emphasised the underperformance of existing diagnostic models for estimating disease probability in patients with stable chest pain. The question arises whether estimates of disease probability should continue to drive the diagnostic process now that anatomical tests are widely available to accurately define disease status. CTCA with a 64-slice (or more) scanner provides objective evidence of coronary disease that is highly sensitive and specific compared with other non-invasive tests. NICE, in its 2010 chest pain guideline,31 made the recommendation that coronary calcium scoring—with CTCA for scores ≥1 should be the investigation of choice for ruling out coronary disease in patients with a low (10%–29%) probability of CAD. The European Society of Cardiology (ESC) guideline followed suit 3 years later, recommending CTCA for patients with a 15%–50% probability of disease.2 These novel guideline recommendations were made in recognition of the ≥94% sensitivity of CTCA for ruling out coronary disease in low-risk populations (table 1). Cost-effectiveness was a key component of the NICE recommendation and has been confirmed in a recent study that concluded that a CTCA-only approach is the most cost-effective diagnostic strategy for the evaluation of patients who have stable chest pain and a low or intermediate probability of disease.32
Unlike the other diagnostic modalities listed in table 1, CTCA has now been the subject of large-scale randomised trials to evaluate clinical outcomes in patients with stable chest pain.33–35 Event rates have been low in these trials and survival benefits are hard to demonstrate although a small reduction in rates of cardiovascular death and myocardial infarction among patients randomised to CTCA was reported in Scottish CT of the HEART.36 In the larger PROspective Multicenter Imaging Study for Evaluation of chest pain trial, there was no demonstrable outcome benefit attributable to CTCA but there was better patient selection for invasive coronary angiography with 72% of patients in the CTCA arm having obstructive disease compared with 48% in the functional testing arm.34 German investigators also found that the diagnostic yield of coronary angiography was increased by prior CTCA,35 a finding further supported by registry data. Thus, among 6 61 063 patients undergoing elective coronary angiography who were enrolled in the National Cardiovascular Data Registry, rates of obstructive disease were 44% with prior perfusion imaging compared with 70% with prior CTCA.37
Recent NICE-approved software developments have extended the functionality of CTCA by providing a non-invasive method of estimating fractional flow reserve (FFRCt) using standard CTCA imaging data.38 In Prospective Longitudinal Trial of FFRCt: Outcome and Resource Impacts, patients in the CTCA cohort who underwent simultaneous estimation of FFRCt showed dramatic reductions to 12% in the rate of normal coronary angiography compared with 73% in the standard care cohort, emphasising the potential value of combined anatomical and functional assessments that CTCA now offers.39
The trial data summarised here have led to recommendations that CTCA should have a greater role in the diagnostic pathway of patients with stable chest pain.40 41 However, some cautions about the clinical application of CTCA need to be acknowledged. Image quality and image interpretation may be adversely affected by a variety of factors, particularly obesity, high coronary calcium burden, cardiac arrhythmias and tachycardia, although recently reported diagnostic sensitivities of 90.4%, 92.7%, 87.4% and 93.7%, in these respective populations, show how improvements in scanner technology have helped deal with these factors.42 As with any procedure using iodinated contrast material CTCA poses the risk of acute kidney injury and preprocedural renal function testing is recommended as well as preprocedural hydration in at-risk subgroups.43 Considerable inroads have also been made into reducing ionising radiation exposure since the original 2010 NICE guidance. A 2014 national audit of CTCA performed in the UK44 demonstrated a median Dose-Length Product (DLP) of 200 mGycm (equating to an estimated dose of 2.8 mSv), comparing favourably to 885 mGycm reported in a similar 50-centre audit published in 2009.45
NICE stable chest pain guideline: 2016 update
Since publication of the NICE 2010 guideline, new evidence has emerged on clinical prediction models of disease probability and the use of non-invasive diagnostic tests. Much of this new evidence has already been discussed in this review and has led to radical changes in the recommendations made for the diagnosis of suspected angina in the 2016 update.46 These changes are summarised in figure 2. Estimates of disease probability are no longer recommended not only because of their inherent unreliability but also because diagnostic testing is no longer dependent on the estimates in patients whose chest pain is assessed as being typical or atypical of angina. Nearly all such patients, regardless of age and gender, have an estimated probability of CAD between 10% and 90% by Genders’ updated prediction model, and CTCA is now identified as the most cost-effective diagnostic test across this range. CTCA is also recommended for patients with non-anginal chest pain if an ECG is done and shows ST-T changes or pathological Q waves. Only if CTCA shows evidence of CAD of uncertain functional significance or is non-diagnostic does the guideline update recommend non-invasive functional imaging, with invasive coronary angiography as a diagnostic back-up if the functional test results are inconclusive.

{kind=link}
{kind=link}
Diagnostic testing for people in whom stable angina cannot be excluded by clinical assessment alone: changes in NICE guideline recommendations 2010–2016. CAD, coronary artery disease; CTCA, CT coronary angiography; NICE, National Institute for Health and Care Excellence.
Of course, increasing CTCA procedures in patients with suspected angina will have resource implications because of the availability of suitable scanners and appropriately trained professionals. The British Society of Cardiovascular Imaging in responding to the NICE guideline update have presented data confirming a lack of CTCA capacity with considerable geographical variation in terms of cardiac-enabled CT scanners and accredited practitioners available to report the scans.47 A nationally coordinated response is now needed to increase capacity and deliver training to dedicated imaging specialists so that the increased demand caused by NICE’s updated recommendations can be met. Meanwhile, NICE predicts that its updated recommendations will lead to considerable annual savings for the population of England, estimates increasing from £6.8 million in 2017/2018 to £17 million in 2020/2021, assuming a complete shift from previously recommended testing strategies to CTCA testing, with 20% of patients going on to have a non-invasive functional test and a further 10% receiving diagnostic invasive coronary angiography. This calculation is based on contemporary National Health Service (NHS) tariffs or recent reference costs and includes modelling for the costs of potential complications of the procedures,48 49 with numbers of patients attending a rapid access chest pain clinic in England each year around 1 20 00050 and pretest probability of CAD proportions derived from recently published data.15 These savings are important given the substantial healthcare utilisation and costs incurred by patients with stable CAD,51 but caution is required in extrapolating the calculated savings to non-UK settings.
The 2016 update to the NICE chest pain guideline marks a radical departure from the earlier diagnostic paradigm that will be welcomed by clinicians. No longer is there the recommendation to apply probability estimates of CAD to guide decisions about non-invasive diagnostic testing. Instead, the new recommendation is for CTCA in all patients with typical or atypical chest pain to determine whether there is obstructive CAD to account for the symptoms. The call for CTCA to have a greater role in the diagnostic pathway of patients with stable chest pain has been answered in the updated NICE guideline.
References
Footnotes
Contributors Professor AT wrote the original version of this paper from start to finish. He also helped with the revisions. Professor CAR developed many of the revisions and helped rewrite the revised manuscript.
Competing interests Prof Adam Timmis NICE guidelines [CG95] Chest pain of recent onset: Assessment and diagnosis of recent onset chest pain or discomfort of suspected cardiac origin. 2010 (Chair) NICE guidelines [CG95]. Chest pain of recent onset guideline update group 2016 (topic expert) Prof Carl Roobottom NICE guidelines [CG95]. Chest pain of recent onset guideline update group 2016 (topic expert).
Provenance and peer review Commissioned; externally peer reviewed.