Article Text

Abstract
Objectives: To evaluate the Swedish model for contact tracing and especially the “Västerbotten model” with centralised, extended contact interview periods, sometimes by telephone.
Methods: Using questionnaires, the contact tracing and interview procedure was evaluated during 2002, followed by an evaluation of contact interviewing by phone in 2005–6.
Results: Patients with diagnosed Chlamydia trachomatis infection reported on average 2.5 sexual contacts, 3.0 contacts when contact interviewing was performed at the clinic, and 2.3 contacts when performed by phone. 65% of the sexual contacts with a known test result were infected.
Conclusion: Centralised contact tracing, exploring the sexual history for at least 12 months back in time, shows good results. Combined with screening of certain risk groups it is probably one effective way of preventing C trachomatis infections. Preventing C trachomatis by primary prevention such as information and counselling is, however, still of great importance.
Statistics from Altmetric.com
During the 1980s the incidence of genital Chlamydia trachomatis reached epidemic proportions in Sweden.1 To prevent an additional increase, C trachomatis was incorporated into legislation on the control of sexually transmitted infections (STI) in 1988. Testing and treatment for C trachomatis are free of charge. Doctors have to report all cases of C trachomatis to the County Medical Officer (CMO) for Communicable Disease Control and to the Swedish Institute for Infectious Disease Control. Contact tracing may be delegated, mainly to a counsellor. Counsellors are found at every sexually transmitted disease clinic, working part or full time with contact tracing. Once notified, the partner is obliged to seek medical advice. If he or she does not show up he or she is reported to the CMO who may force testing.2 Prescription of antibiotics without previous testing is not allowed. Regular partners are always treated.
After introducing these measures the number of C trachomatis cases fell 54% (1989–94). The incidence of complications also decreased.3 4 Despite all efforts the incidence of C trachomatis increased 138% from 1997 to 2005.1 A slight decrease in 2006 was probably caused by a new variant of C trachomatis that could not be detected by the main nucleic acid amplification tests used.5 The Swedish model has been questioned and contact tracing and opportunistic screening have been criticised as being expensive and less effective than systematic screening.1 6
The C trachomatis case rate in Västerbotten has increased 155% between 1997 and 2006; nevertheless it was the second lowest in the country in 2005 and in the beginning of 2007.4 If the epidemic phase is defined by secular trend data only, there are often significant artefacts.7 The introduction of superior tests for C trachomatis (PCR/ligase chain reaction) in 1996 and a 49% increase in analysed tests from 1998 to 2006 may explain some of the increasing incidence as do changes in sexual behaviour.8 In contrast to other areas of Sweden, contact tracing in Västerbotten is highly centralised. Furthermore, in Västerbotten, the sexual history is explored for 12 months, compared with the six that has been standard in most of Sweden. We therefore wanted to investigate whether the lower incidence is a result of centralised and extensive contact tracing. The recommendations from the National Board of Health and Welfare are now changing, in accordance with our results.9
As Västerbotten is sparsely populated, contact interviewing by phone was initiated to facilitate tracing in remote areas. Increasing numbers of patients prefer phone interviews. In the second part of the study we therefore wanted to evaluate phone interviews compared with interviews at the clinic.
METHODS
Västerbotten comprises approximately one-eighth of the area of Sweden but only 3% of the population. The average age of the inhabitants is lower (approximately 10% between 18 and 24 years, compared with 8%) and 70% of the inhabitants live in the two largest cities Umeå and Skellefteå (112 000 and 72 000 inhibitants, respectively).10 Four counsellors were responsible for the main part of contact tracing, each performing these 6–30 h per week. The rest was performed by nurses, doctors, midwives and other social workers. All samples were tested at the laboratory at the University Hospital, Umeå, using nucleic acid amplification technology.11
In the first part of the study, all cases of C trachomatis reported to the CMO during one year (2002) were included. The contact tracer signing the report was asked to complete the study questionnaire. The questionnaires included questions regarding: profession of the tracer; period of sexual history evaluated; number of contacts; whether the patient had received information about abstinence until the test result was available and, if tested positive, until finishing antibiotics; whether the identities of the contacts were known; time of last intercourse; whether the contacts had been requested to take a test; had been tested and, if not, whether they had been reported to the CMO; the contacts’ test results and whether the partner had received antibiotic therapy without testing. No directions regarding contact tracing were given. All questionnaires returned before 1 April (2003) were included.
The term “index” was used for the patient and “contact” for the sexual partners. Partners were categorised into groups corresponding to time of last intercourse with the index. In the second part of the study a questionnaire was filled in by the contact tracers doing most of the interviews between November 2005 and December 2006. These questions concerned partners and whether the contact interview was performed by appointment or by telephone, with the objective of investigating the possible differences. No questions were asked about partners’ test results. The patients themselves chose to be interviewed either by phone or in person. Partners were asked by contact tracers to seek medical advice and were obliged to confirm that they had. Once again, no directions about the contact tracing were given.
RESULTS
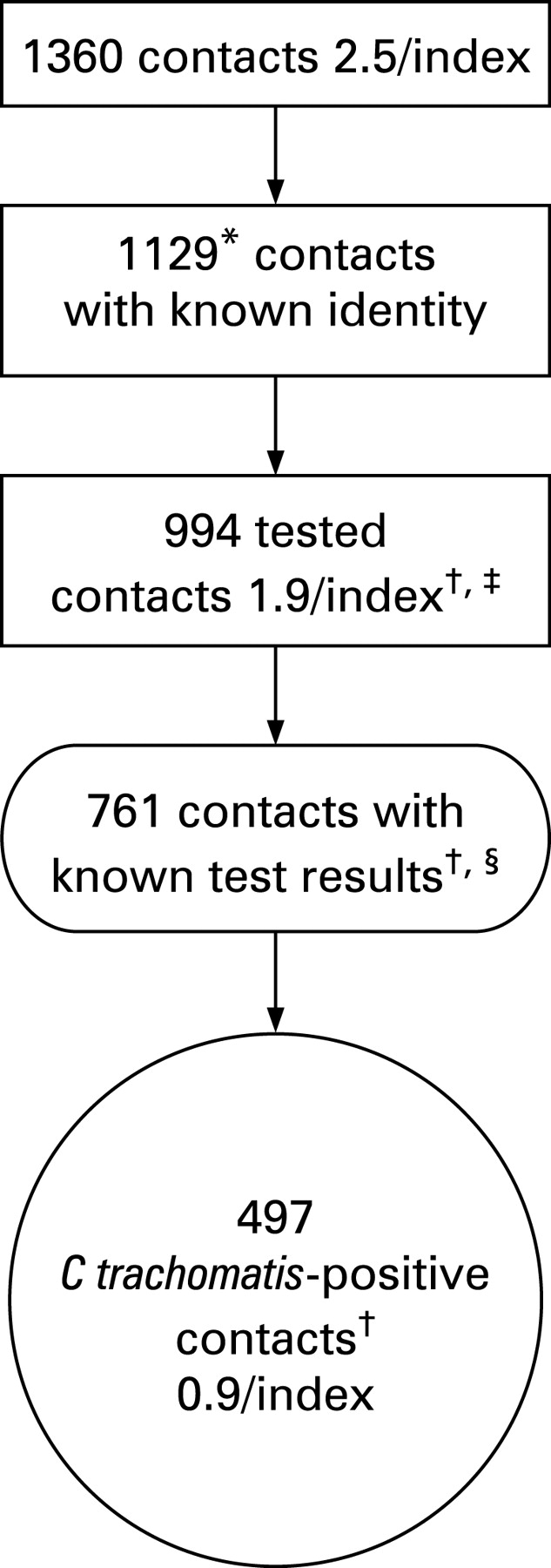
In 2002, 550 C trachomatis-positive patients were reported to the CMO. A total of 544 questionnaires was sent to the tracers and 534 were completed and returned (98%). Fifty-five per cent (294) of the indexes were women. The mean age of the indexes was 23.8 years (range 15–57), 89% (479) were aged 15–29 years. The 534 index patients reported in total 1360 sexual partners (average 2.5 contacts/index). Sixty-seven per cent (360) of the index patients had two or more partners and 22% (116) had four or more partners. For women, the average was 2.6 partners per index, 71% (208) had two or more and 24% (70) had four or more partners. For men, the average was 2.4 contacts per index, 63% (152) had two or more and 19% (46) had four or more partners; 0.9 C trachomatis-infected partners per index were identified. In 1255 cases (93%) the time of last sexual intercourse was known. Fifty per cent of the reported contacts last had sex with the index in the two months before the index’s diagnosis. The numbers of partners decreased with time since last intercourse. Only four indexes had their most recent sexual contact more than 12 months before diagnosis (table 1). Seventy-two per cent of the infected partners with a known test result belonged to group 0–2, 20% to group 3–6, 6% to group 7–12 and 2% to group ⩾12. The percentage of partners who were infected generally declined with time since last intercourse with the index.
Fifty-four per cent of all contacts in group 0–2 were infected, 28% in group 3–6, 13% in group 7–12 and 68% in group ⩾12 were infected.
The results differed between tracers of different professions, as did patient demographics. The indexes reported 2.5 partners on average. The patients of the counsellors and the patients seeing the midwives reported the highest numbers of partners, with means of 2.6 and 2.5, respectively (table 2). Fourteen tracers, 11 of whom were doctors, performed only one contact interview during the year. Their patients reported 1.3 partners per patient and 40% did contact interviews covering the previous 12 months. Contacts were elicited for more than 12 months for only 34 indexes and they reported 1.3 contacts per index.
Interviewing at the clinic or by phone
From November 2005 to December 2006 six tracers had 567 patients, all of whom were included in our analysis. Seventy-eight per cent (441) of the interviews were carried out by two persons. Although the index patients chose whether they wanted an interview at the clinic or by phone, the groups were quite similar (table 3). Some index patients reported foreign partners (phone tracing at least 27 partners, clinic tracing at least 31) and, in compliance with Swedish regulations, no attempt was made to contact these individuals, who are included in our analysis. One index, interviewed by telephone, did not mention his contacts and was excluded from the summary. There was no significant difference between the methods (Student’s t test) on any variable.

{kind=link}
DISCUSSION
During 2002 contact tracing in Västerbotten was centralised and 78% of the interviews were performed by four experienced counsellors. On average 2.5 contacts per index were reported (1.4–2.2/index in other Swedish studies12 13). More experienced staff tended to elicit more partners, in accordance with Eitrem et al.13 The characteristics of the patients varied between the professions, which might have influenced the findings. The midwives’ patients were mostly young girls whereas the doctors’ patients were mostly men and were slightly older. Most of the midwives and counsellors used notification periods of 12 months or more. Few of the doctors and persons doing only one interview used 12-month notification periods, which of course affected the outcomes. We found that 65% of the tested partners with a known result were C trachomatis infected. The number of reported and infected contacts was highest among those with whom the indexes had intercourse shortly before diagnosis. Seventy-nine per cent of the contacts with a known test result and who had had intercourse with the index patients 0–2 months before the index was tested were positive for C trachomatis. In the group of contacts having intercourse with the index 7–12 months before testing, 30% were positive. Reasons why more partners are reported at the beginning could be that partners in a relationship may be more likely to be in group 0–6. Contacts from long ago may be somewhat more likely to be forgotten or repressed.14 If the notification period is longer more of the sexual history is revealed and more partners are probably reported. The incubation time for C trachomatis is approximately 7–14 days. Individuals with symptoms probably came for testing earlier and the contacts were therefore more likely to belong to group 0–2. C trachomatis infection may clear spontaneously or persist.15 16 The precise proportions of infections cleared is unknown and this aspect may affect the outcome of our study. Only 15 contacts belonged to the group of 12 months or greater and 73% of those with known test results were C trachomatis positive. According to the tracers, notification periods of more than 12 months were often used when the regular interval did not include the most recent partner. This could explain the small total number of partners in the group ⩾12 and the high number of infected partners. An exact figure for the length of the notification periods can not be given. It seems that the longer they are the more partners are found. In group 7–12, however, 30% of the patients with a known test result were infected. This could be compared with the prevalence of C trachomatis among asymptomatic women in Europe, which is 1.7–17%, depending on the setting, context and country.17 In Sweden, the prevalence of C trachomatis among men and women is 1.1–10%, depending on the group tested.18–20
Key messages
Contact tracing is important in finding individuals infected with asymptomatic STI and may limit the complications.26
Extended interview periods back to 12 months before diagnosis yield many infected partners.
Patients of experienced tracers reveal more partners. We therefore recommend centralised contact tracing.
Patients of experienced contact tracers also reveal a high number of contacts during an interview by phone. This could be a good option in remote areas and if there are difficulties in setting an appointment at the clinic.
Although most partners belong to group 0–2 months, if exploring the sexual history for only 90 days many infected partners would be missed. These individuals probably play an important role in the continued transmission of C trachomatis.21 Pioneer work was performed by Zimmerman-Rogers et al,21 indicating that the notification period should be at least 180 days. Our work confirms the importance of extended notificaton periods and also points out that in group 7–12 the number of partners and infected partners is still high. Extended notification periods are also resource demanding but the fact that 30% of the partners belonging to group 7–12 are infected can not be overlooked. The screening of certain risk groups might be an alternative, or even better a complement and has shown good results.22 23 Screening is, however, also resource demanding. The advantage of contact tracing is that many contacts are identified, tested and treated, irrespective of factors such as age, place of residence and number of partners. Based on our figures it seems that testing and treating only the most recent partner is insufficient because indexes report on average 2.5 contacts per year. We therefore recommend centralised contact tracing and interviews performed by experienced staff in combination with limited screening of groups at high risk and primary prevention methods. For example, retesting of C trachomatis-infected patients shows good results.24 These approaches must be combined with public health information. It can be difficult to encourage people to attend clinics for contact interviews and contact tracers spend much time trying to make appointments. It is therefore of the utmost importance that the contact interview procedure is kept as simple as possible.25 In Västerbotten slightly more contacts are reported when the contact interview is performed at the clinic; however, the figures in our phone group are higher than in other contact tracing studies.12 13 Patients with many partners were encouraged to attend the clinic and that is one reason why more partners were reported in that group. Patients may feel more anonymous if interviewed by phone as one may lose dimensions in the conversation used to create trust and convey the importance of the tracing. It is probably even more necessary to be experienced in tracing and telephone skills if interviewing is performed by phone.
CONCLUSION
“The Västerbotten model” for contact tracing fulfils these criteria and may function as a model for contact tracing. Combined with primary prevention and screening of certain risk groups it could be an effective way of preventing C trachomatis epidemics.
Acknowledgments
The authors would like to thank the contact tracers in the county of Västerbotten for their participation.
REFERENCES
Footnotes
Contributors: JB, BG and AÖ contributed to the original idea; HC, JB and EN designed the study; HC collected the data; HC, JB and EN analysed the data and contributed to writing the paper.
Competing interests: None.