

Fournier gangrene (FG) can present subtly and have devastating consequences if not discovered at an early stage. Primary care providers must be aware of this fulminant, necrotizing, albeit rare, infection that affects the perineal, genital, and perianal regions, as it can be mistaken for other common benign conditions but can progress rapidly to multiorgan dysfunction and death if missed.1 A high degree of suspicion should be maintained in those with risk factors such as diabetes, trauma, alcohol use disorder, obesity, hypertension, HIV infection, and other immunosuppressed states. Surgical debridement is the mainstay of treatment, along with early use of broad-spectrum antibiotics. Nonetheless, the mortality rate continues to be high.2,3
This article describes the case of a middle-aged man who presented to a community emergency department with progressive perianal swelling and pain and systemic symptoms suggestive of early FG. A comprehensive PubMed search of the MeSH terms Fournier’s gangrene, necrotizing infection, perineal, and perianal was conducted for medical literature spanning January 1996 to April 2015. We reviewed all relevant observational studies, cohort studies, randomized controlled trials, and review studies with more than 25 patients published in the past 5 years.
Case
A 46-year-old man with a history of non–insulin-dependent type 2 diabetes mellitus, dyslipidemia, and hypertension presented to a busy community emergency department at the suggestion of his family physician for management of a possible perianal abscess. He described a 1-week history of worsening perianal pain, swelling, and chills. On further questioning, he denied any history of abdominal surgeries, recent perianal interventions, or trauma. A review of systems had no relevant findings, with no relevant past medical or family history. He was in a monogamous heterosexual relationship. His medications included atorvastatin, diltiazem, gliclazide, irbesartan, and metformin, with no recent changes.
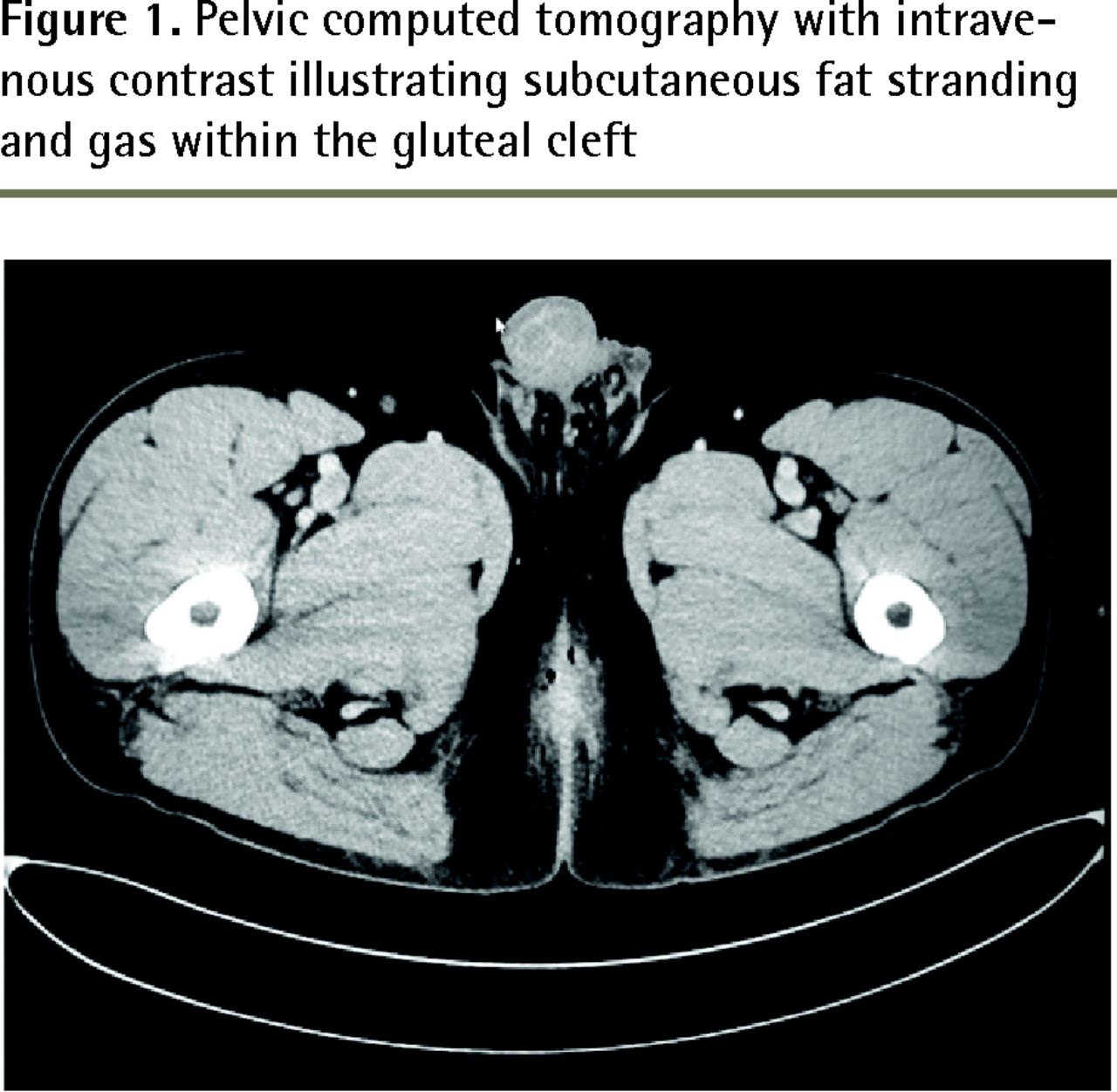
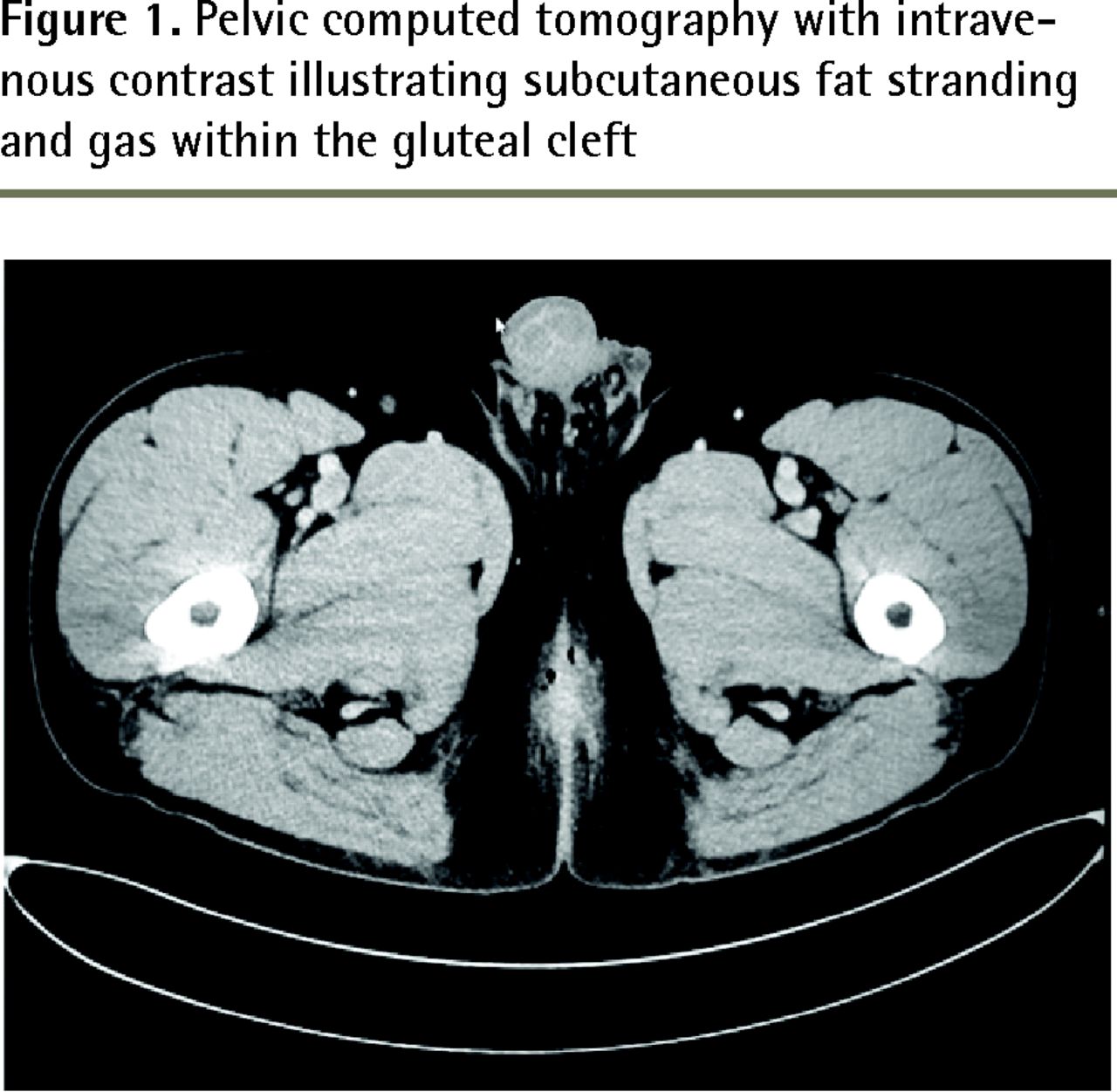
On examination, the man appeared to be quite uncomfortable and febrile, with a temperature of 38.6°C. His heart rate was 112 beats/min and his blood pressure was 160/89 mm Hg, with an oxygen saturation of 95% on room air. The findings of his head, neck, cardiovascular, and respiratory examinations were unremarkable. His abdomen was soft, nondistended, and nontender. The ischioanal fossa and perianal region were found to be erythematous and indurated bilaterally, although there was no appreciable fluctuation or crepitus. They were extremely tender to palpation and there was some extension of the erythema and induration toward the scrotum. Findings of a digital rectal examination were negative for any palpable masses. Baseline laboratory investigations were performed, including a complete blood count, blood cultures, and measurement of electrolyte, creatinine, and lactate levels. The white blood cell count was elevated at 15.9 × 109/L (neutrophils 11.4 × 109/L), the lactate level was 1.0 mmol/L, and the rest of the results were unremarkable. Given the extent of the findings and the concern about a deep-seated infection, computed tomography (CT) of the pelvis was performed with intravenous (IV) contrast. This revealed subcutaneous fat stranding and gas just deep to the gluteal cleft involving the urogenital and anal triangles of the perineum, suggestive of FG (Figure 1). The general surgery, urology, and plastic surgery services were consulted immediately, and the patient was booked into the operating room for urgent exploration. He was given 4.5 g of IV piperacillin-tazobactam every 6 hours and 900 mg of IV clindamycin every 8 hours in the interim.
On initial exploration, the tissues appeared edematous but there was no necrotic tissue or purulent discharge noted. The ischioanal incisions were packed and the patient was transferred to the intensive care unit for observation and possible re-exploration given the risk of rapid progression. On postoperative day 2, the patient continued to have substantial induration and tenderness and was taken back to the operating room. Larger incisions were made, this time revealing purulent discharge and gas. Drains were left in place and the patient had substantial improvement of his symptoms postoperatively. He was deemed ready for discharge on postoperative day 4 and was instructed to take 500 mg of oral ciprofloxacin every 12 hours and 500 mg of oral metronidazole every 8 hours for 7 days with analgesia; sitz baths, stool softeners, and home care for his drains were also recommended. Ultimately, this case likely represents early progression toward FG given the changes noted on CT and clinical features that were recognized expeditiously.
{kind=link}
Pelvic computed tomography with intravenous contrast illustrating subcutaneous fat stranding and gas within the gluteal cleft
Discussion
The initial description of FG is credited to the venereologist Jean-Alfred Fournier, who observed this fulminant gangrene affecting the penile and scrotal tissues of young men.1 A recent large cohort study that reviewed 120 cases of FG found the most common nidus of infection to be the gastrointestinal tract (49.2%). Other sources were the genitourinary tract (43.3%) and skin (7.5%).4 The most commonly cited comorbid risk factors are diabetes, body mass index greater than 30 kg/m2, hypertension, end-stage renal or liver failure, smoking, alcohol abuse, and immunosuppressed states.5,6 Fournier gangrene also has a clear predilection for men and is by and large a polymicrobial infection. Escherichia coli, Bacteroides, Staphylococcus, and Streptococcus are commonly isolated from cultures, as they are typical perineal commensal organisms. Anaerobes other than Bacteroides are less frequently isolated but organisms might include coliforms such as Klebsiella, Pseudomonas, clostridia, and Corynebacterium.7,8 Pathogenesis is purported to be a suppurative bacterial infection causing enzymatic activation, platelet aggregation, and inflammatory reaction leading to microthrombosis of local subcutaneous vasculature and tissue destruction.1 Clinically, FG often presents as indolent cellulitis near the portal of entry and rapidly progresses to swelling, dramatic pain, and systemic features. Crepitus might be observed if gas-producing organisms are involved. The infection spreads along fascial planes from the perianal and perineal regions toward the thighs and abdominal wall; however, the testes are typically spared, as their blood supply originates from the abdominal aorta.5 While typically a clinical diagnosis, imaging techniques such as bedside ultrasound to look for subcutaneous air, CT, or magnetic resonance imaging might be used to confirm the diagnosis in uncertain cases.9–11
A scoring system called the Fournier’s Gangrene Severity Index might be helpful in determining outcomes; however, the most important features in determining mortality are systemic inflammatory response syndrome criteria and perturbations in basic biochemical markers including complete blood count, lactate level, creatinine level, blood urea nitrogen level, and electrolyte levels.12–15 Along with early use of broad-spectrum antibiotics, aggressive and early surgical debridement has been the mainstay of treatment for FG.1,9–11 Imaging should not delay surgical intervention if a clinical diagnosis can be made, as this condition can progress very rapidly. To differentiate FG from a simple soft tissue infection, the Infectious Diseases Society of America recommends clinicians look for findings such as persistent, severe pain; bullae; skin necrosis or ecchymosis; gas in the soft tissues; edema that extends beyond the margin of erythema; cutaneous anesthesia; signs of systemic toxicity; and rapid spread, especially during antibiotic therapy.11 Treatment might involve a multidisciplinary team of urologists, plastic surgeons, and general surgeons, and monitoring in an intensive care unit. When in doubt regarding the diagnosis, consultation might be beneficial, as surgical exploration will provide both confirmation of the diagnosis and definitive treatment. Multiple surgical debridements are often required (2 to 4 on average) to remove all necrotic tissue.1,9 Initial treatment should also involve aggressive resuscitation with IV fluids for any hemodynamic instability and early administration of broad-spectrum antibiotics (piperacillin-tazobactam; clindamycin for antitoxin effects against toxin-elaborating strains of streptococci and staphylococci; and vancomycin for methicillin-resistant Staphylococcus aureus coverage).7,10,11 Hyperbaric oxygen treatment might also be considered as an adjunct if available.7,10,11 Fournier gangrene continues to be a devastating condition, with mortality rates ranging from approximately 2% to 20% in recent literature.1–4
Conclusion
Despite clinical advances over the past century, FG continues to be an important cause of death in ambulatory patients who present to primary care providers with what appear to be uncomplicated soft tissue infections. It is vital for primary care providers to suspect FG in patients with associated risk factors and features out of proportion to local findings (eg, severe pain, rapid progression, signs of systemic illness). In those with possible FG, consultation with surgical specialists and early transfer from remote sites for definitive management have proven to be life saving.
Notes
EDITOR’S KEY POINTS
Fournier gangrene (FG) should be considered in patients with risk factors such as diabetes mellitus, obesity, vascular disease, end-stage organ failure, and immunosuppression who present with systemic symptoms and severe perianal or perineal swelling that is out of proportion to what would be expected with a simple subcutaneous abscess.
Imaging methods such as ultrasound, computed tomography, or magnetic resonance imaging might be used to look for features suggestive of FG if the diagnosis is unclear, but should not delay definitive surgical management. Mortality is high in patients presenting with FG; early diagnosis can be life saving.
While surgical debridement is the mainstay of treatment of FG, primary care practitioners should also ensure that patients receive early broad-spectrum antibiotic coverage, intravenous fluids if there are signs of hemodynamic instability, and appropriate resuscitative measures.
POINTS DE REPÈRE DU RÉDACTEUR
La gangrène de Fournier devrait être envisagée chez les patients ayant des facteurs de risque comme le diabète, l’obésité, une maladie vasculaire, une défaillance d’organe en phase terminale ou une immunosuppression, et qui présentent des symptômes systémiques de même qu’une enflure périanale ou périnéale grave et disproportionnée par rapport à ce à quoi on s’attendrait avec un simple abcès sous-cutané.
Si le diagnostic n’est pas évident, on peut recourir à l’imagerie comme l’échographie, la tomodensitométrie ou la résonance magnétique pour détecter des caractéristiques propres à la gangrène de Fournier, mais la démarche ne doit pas retarder la prise en charge chirurgicale définitive. La mortalité est élevée chez les patients atteints de la gangrène de Fournier; le diagnostic rapide peut sauver la vie du patient.
Si le traitement de la gangrène de Fournier repose principalement sur le débridement chirurgical, les médecins de soins primaires doivent aussi assurer que les patients reçoivent rapidement des antibiotiques à large spectre, des liquides par voie intraveineuse s’ils présentent des signes d’instabilité hémodynamique et des mesures de réanimation appropriées.
Footnotes
This article has been peer reviewed.
Cet article a fait l’objet d’une révision par des pairs.
Competing interests
None declared
- Copyright© the College of Family Physicians of Canada
References
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.